The relationship between transmission rate (“R”) and heat/humidity is an aspect that I have tried to read up about more. If for no other reason than that Indonesia is a hot and humid area, and something to hang my hopes on.
I have seen that paper which the NYT quotes, and I think there may be some weak evidence that heat/humidity indeed reduces R, but that paper is a bit problematic b/c the variance is too high.
Also unclear is how much the lower transmission in hotter countries are due to them almost universally being poor and poorly governed, leading to reduced/no testing. For example, Indonesia (270 million people) has done as of today 2,756 tests (10/million), with 579 positives (21% positive rate), which is abysmal.
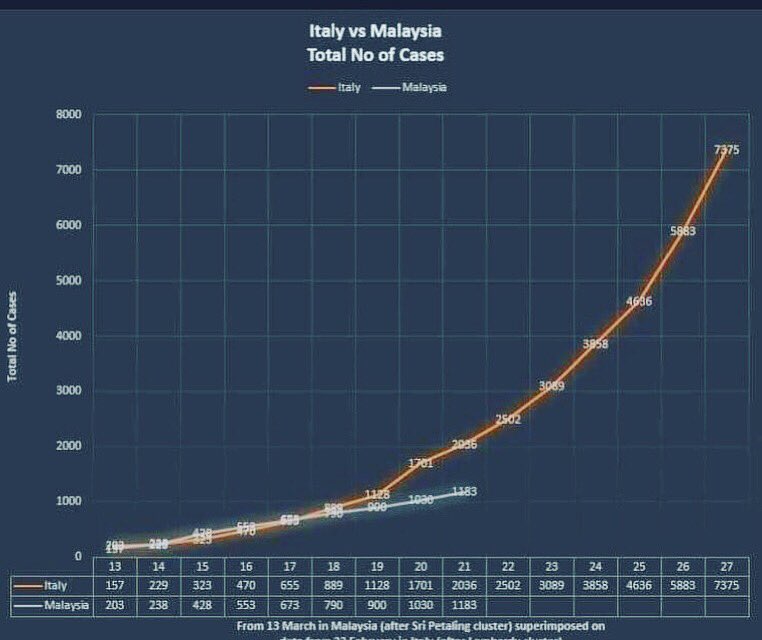
A better situation in Malaysia (32 million people), a country next to Indonesia, with about the same demographics and climate. They have until last evening done 17,923 tests (560/million), with 1518 positives (8.47% positive rate). Below is a graph comparing Malaysia’s case growth rate vs Italy, beginning from when both had 100+ cases.
The graph is from March 21, but even if you extrapolate the data March 23, it is still a linear growth rate. Furthermore, around 900 of the cases in Malaysia can be attributed to a single religious gathering. As these countries are now testing more and more, we can probably begin to really draw conclusions about heat/humidity effects in transmission rates.
Edit to add: Another mechanism by which respiratory diseases are slowed is apparently via small daily doses of Vitamin D (there was that MedCram video that showed robust evidence for this). Well one perk of living near the equator is that you do get small daily doses of Vit D just from being in the sun for a few minutes every day, but this too will be the case for the northern hemisphere when summer comes.
If you want to translate a potential number of infected people into a potential number of dead people, you simply have to have the ratio between the number of people who die and the number of people who are infected, which is not the same as the number of people who die divided by the number of people who are confirmed positive. I’m sorry if you don’t know the correct number, but not knowing the number means you can’t project how many people will die from an estimate of how many people will become infected. You can’t just use a different number because it’s easier to come up with.
Also, we do have a not-hopelessly-biased estimate of the infection fatality rate, which is 1.25% from the Diamond Princess. That is likely to be an overestimate due to about 30% of the cruise ship population being 70+, which is the demographic that accounted for all of the deaths. More here*:
*Based on this source, it seems that there have been two more deaths among the passengers. That’s factored into the 1.25% number above, but not in the paper linked above, although that paper used some kind of statistical correction to estimate future deaths.
Based on the estimated IFR of 0.5% from that paper and 60% of New York state’s population getting the disease (r0 = 2.5), you would expect 59,000 people to die.
I don’t get how you’re missing the point this thoroughly.
If you want to translate a potential number of infected people into a potential number of dead people, you simply have to have the [ACTUAL CFR UNDER CIRCUMSTANCES OF HEALTHCARE SHORTAGE], which is not the same as [THE CFR YOU GOT FROM THE DIAMOND PRINCESS WHERE EVERYONE GOT TREATMENT]. I’m sorry if you don’t know the correct number, but not knowing the number means you can’t project how many people will die from an estimate of how many people will become infected. You can’t just use a different number because it’s easier to come up with.
FYP.
To come at this from a different angle, countries like Germany and South Korea currently have a CFR which is like 18 times less than the CFR in Italy. What’s your explanation for this? All these countries are undercounting cases, right? Is Italy undercounting more cases by a factor of 18?
The fact that the CFR is radically worse under conditions of equipment shortage is a lot more important than whether the “real” CFR if people receive good treatment is 0.3% or 1%. That’s an almost irrelevant factor in comparison.
CFRs below 1% are achievable, but it requires having enough ventilators and testing well. I’ve got the lower bound for true fatality percentage in Italy at 2.5%.
The average age of people who have died in Italy is 78.5-79.5 from the two sources I’ve seen. Less than 5% of the population is over 80. There’s no way the true fatality rate is 2.5%. There are a LOT of young asymptomatic, or nearly asymptomatic, people.
I’m not in California but I have pulled off job I was in the middle of in portland. I was hoping they wouldn’t allow construction but it seems they are. Homeowner who said he had a fever and that he was quarantining himself for 3 days(not sure why he decided 3 days) is now demanding I come back and finish.
I read somewhere that the percentage of Italy’s population over 65 is 23%. Guessing that 10% are aged 70-79 and 5% aged 80+, if you look at the CFRs for those age groups in Italy, that would give a whole-population CFR there of 2.25% even if nobody under 70 died. You can’t dodge this by proposing undetected young cases, you have to assume that there are widespread covert cases of 70+ year olds as well.
To get 2.5%, you have to assume that 70% of infected aren’t known and that no one currently alive with the virus dies. The best estimates I have seen are 20-50% are asymptomatic.
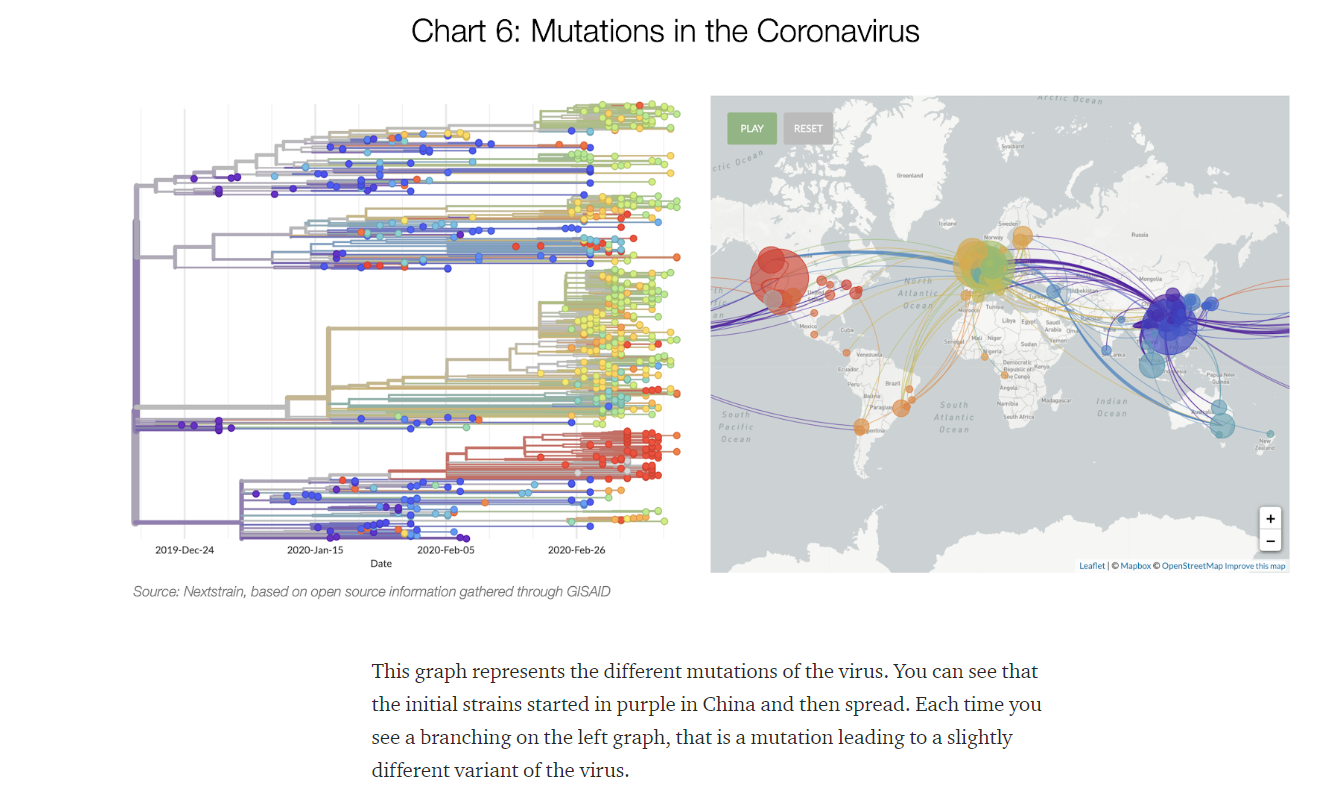
Yeah, but according to this very excellent article (seriously, the best I’ve read so far, grunching a bit so it may have been posted before) the virus has already mutated multiple times:
The CFR maps from detected cases to deaths. You can’t use it to map from infections to deaths unless you know how many infections give rise to detected cases. And if you want to use Italy’s CFR specifically, you need to know how many infections give rise to detected cases when the medical system is overloaded. But you don’t know that number.
The anomalies in the data that you’re pointing out actually make it clear that there are denominator shifts going on from country-to-country. Italy had 28k cases on March 18, and 3k deaths. Germany has 29k cases and 123 deaths. Italy crossed the 123 death mark on March 5, with 3300 active cases. There’s a 10x disparity right there that can’t be attributed to ventilator shortages.
I’ve never been to San Fran, but comparing NYC and LA, if would obviously spread faster in NYC. More widespread use of public transit, less space in the city keeps people in smaller spaces, tiny apartments, packed bars and restaurants and weather that keeps people inside. LA is more of a driving city, has mote space, and people can spend more time outside.
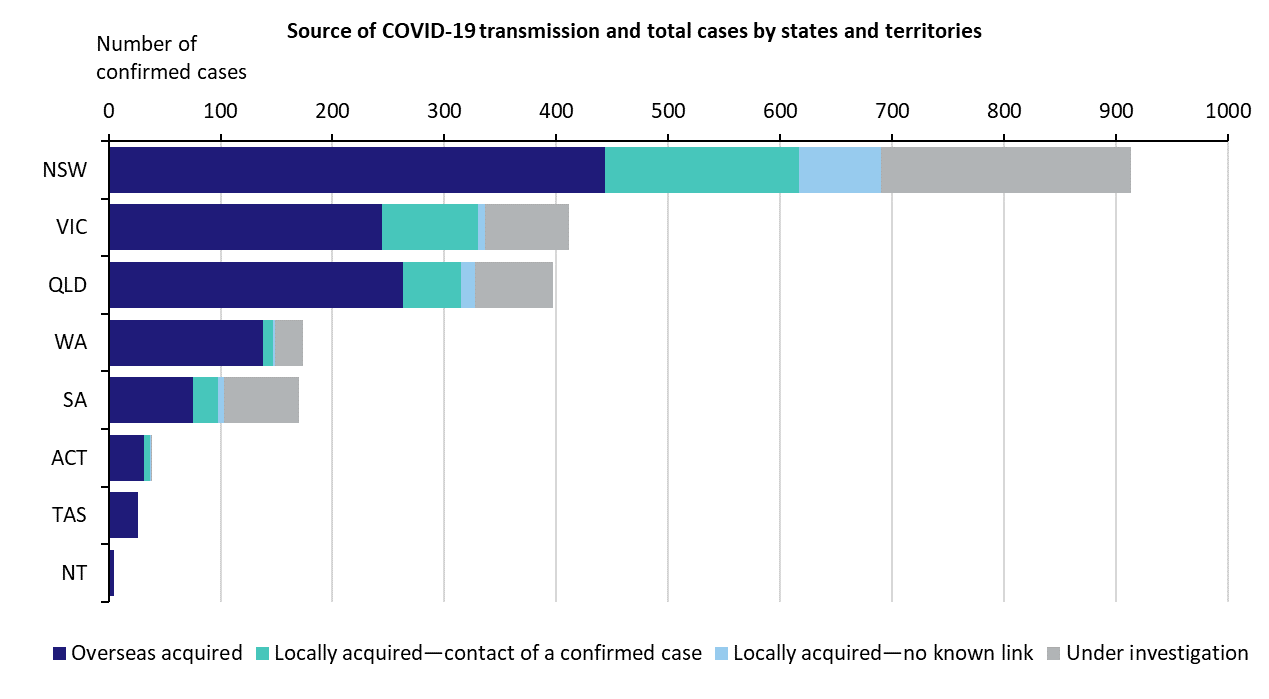
At least you are not living in Sydney. I am so glad I can work from home indefinitely because Sydney needs a total lockdown now. I am definitely only going to the local supermarket and nowhere else. Only risk comes through my wife who for some reason still needs face to face meetings.
My buddy drove by the Koch brothers’ properties on Palm Beach Island this weekend, and they all had guards stationed outside. Yeah, rich assholes are going to force everyone else to get back to work with an elevated risk of sickness and death, business as usual, and they are going to stay isolated and protected (In palatial fortresses they built with our money)while they continue to suck away the vast majority of the fruits of everyone’s labor.