As Churchill hinted at, reasons to think this particular strain wouldn’t cause less illness and, in fact, would be more resistant to treatments and possibly evade vaccines much more meaningfully than we have seen from prior strains.
We’ll have to see. I’m still not panicked because this variant is still a dog to become the dominant one. Worth monitoring and meaningful chance one of these will send us back to quasi lockdown mode at some point if we continue our let it rip course and it appears before vaccine 2.0 tech comes out.
Goes without saying that delta plus transmissibility plus evades current treatments would be a total disaster as it would require real extended actually lockdowns (not US style lockdowns) worldwide, so don’t mean to downplay this. But wouldn’t plan to be locked down for half of 2022 just yet.
EDIT: oh missed the last piece talking about delta with fewer symptoms. That’s sort of a mixed bag, usually more transmissibility with slightly better symptoms bad for the population.
Or everyone can just take a rapid test before going to the house in the first place? Yeah these extreme measures that nobody is going to follow are not helping. I’m not really sure what extra utility is gained by making everyone test in the garage first instead of before they leave home.
That garage part was just one of the guests saying things. Good example of why talk show hosts shouldn’t be the ones responsible for guiding the populace through the holidays. When you have leadership whose approach to COVID is take a vaccine and we need to have COVID behind us for political reasons, we are unfortunately left with talk show hosts to guide us.
The leadership wants COVID behind us for political reasons, and yet the RWNJs are lampooning the leadership for still upending everyone’s lives over this “charade,” in the words of one responder.
You obviously know this, but I found it a bit counterintuitive that different virus strains aren’t really competing directly, like good bacteria in your gut might keep pathogens out by gobbling up all the available nutrients. At any given time, only a tiny percentage of people are actively infected. The damping effect that one strain has on another is through the immune response. Immune people are a different habitat from naive people are different from vaccinated people.
Delta is the champion of r-selection, and has evolved to immediately grab naive/waned hosts as soon as possible. It’s possible (maybe? You tell me) that we could see a more k-selected variant that has enough immune escape to replicate in human habitats that are inhospitable to Delta (vaccinated people, people with some waning but not enough to let Delta in). In that scenario, hypothetical variant could be a big problem as long as it’s growing at all, even if it’s not growing relative to Delta. Early on in the exponential growth curve the absolute numbers are a rounding error, but eventually they’ll explode if the carrying capacity is large.
It seems plausible that this is a scenario where having an out-of-date strain in the vaccine might be a problem. The circulating virus is already significantly different from the vaccine strain, so it stands to reason that it might need fewer mutations to achieve a high degree of escape, which might not be true if the vaccine was against Delta specifically. A corollary is that Delta infection might be more protective against hypothetical variant than the vaccine? It’s also unclear to me what happens when a vaccinated person is exposed to, but doesn’t get infected with Delta. Does your immune system get triggered enough to look for new antibodies, or does it just crank out vaccine-strain antibodies until it snuffs out the exposure, then move on with life?
To last 30 days. Right now, a full lockdown is not on the table. But at the same time, a state of emergency wasn’t on the table yesterday. So who knows? Right now, it’s restrictions on open/close hours for businesses and on the upcoming Christmas market. It’s also acknowledged that mandatory vaccination for some professions is inevitable. But it’ll be such an unpopular opinion that I imagine he’ll leave that decision to the incoming government. It’s projected that the number of hospitalizations will surpass the current record in two weeks.
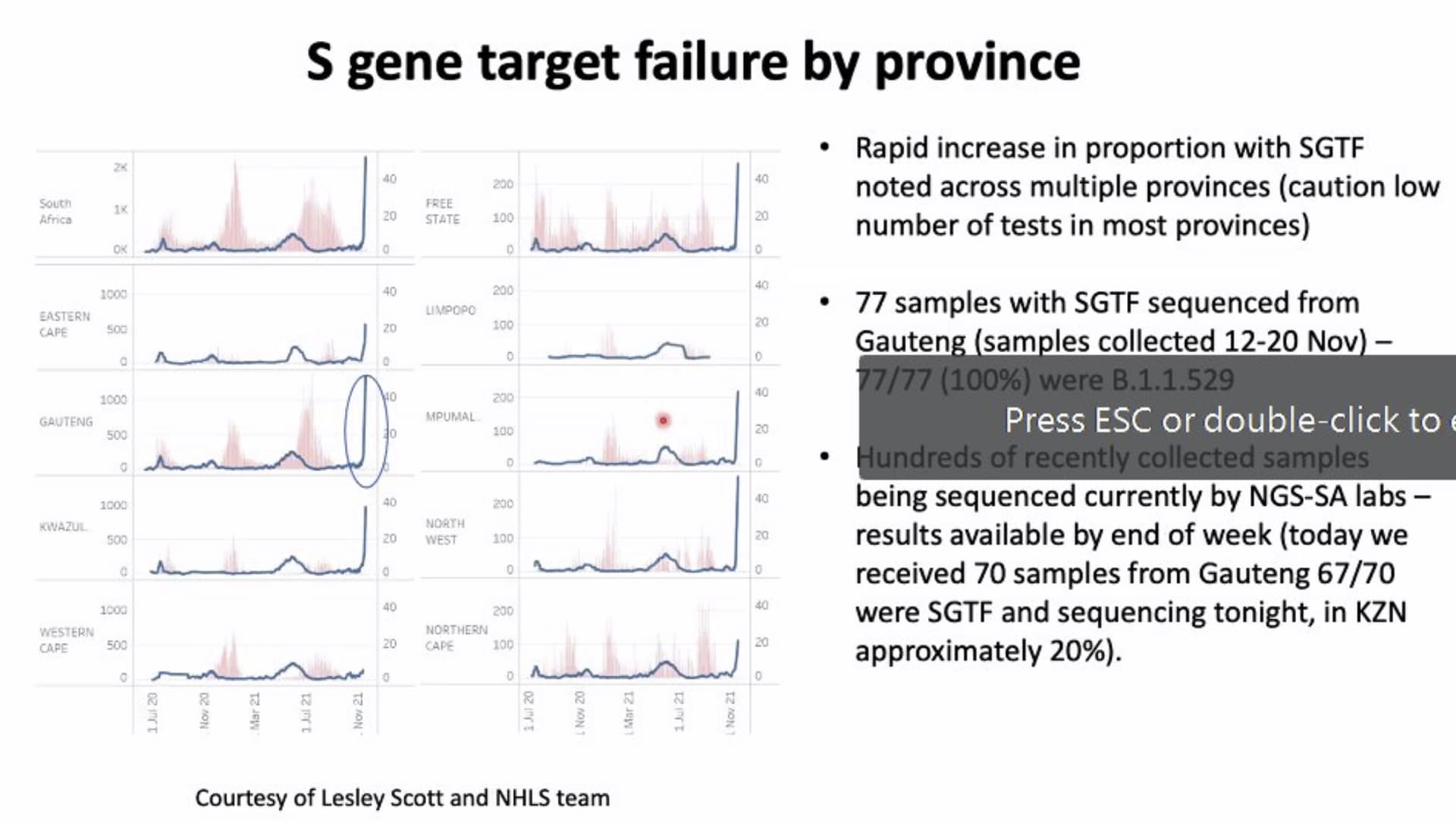
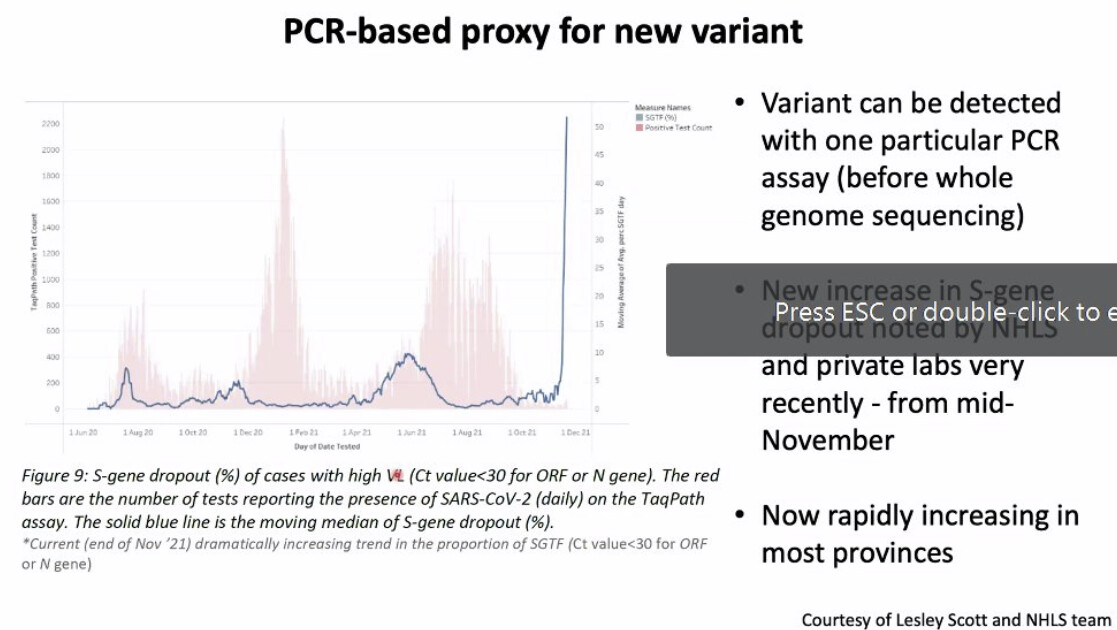
Sounds like B.1.1.529 will get a Greek name tomorrow.
Just got my first taste of MRNA (booster) and now learn the ~32 spike mutations may (I dunno but there is concern) be problematic for those type of vaccines - AZ booster next please!
The Hong Kong returnee testing negative on his pre-flight PCR and postive a few days later on quarantine test which kinda implies B.1.1.529 has already travelled far and wide and will continue to do so - I seriously doubt the UK will reimpose quarantine hotels for all too soon and, obviously may already be too late.
I’m not sure how the immune system reacts to an antigen with some 25% reactivity with the existing antibodies. I suspect the immune system generates a range of antibodies and the “best” one is selected to be mass produced. (Based on binding strength). Immunology class was a long time ago.
But In the interim, having some antibody action should slow down the new strain if it’s not completely evasive.
So have binding constants between antibody and antigen (spike protein) and between the spike protein and the host receptor (ace2). We have raw replication rates. We have efficiency of getting inside the cell once the receptor is grabbed, we have vaccine immune response, we have previous infection response, we may have more than one variant in a host. And then there are the issues of morbidity and host range….
In summary it gets to be quite the complicated equation.
But the more we have spread both generating variants and contact with partially immune folks we are primed for selecting something bigger and badder.
If it wasn’t so effing complicated politically and regulatory it would be great to update a booster twice a year. I suspect the best we will manage is once per year unless something changes drastically.
Spike proteins are what viruses use to get into human cells, and some of the vaccines work by training the body to recognise the spikes and neutralise them.
Mutations on the spike can therefore potentially prove problematic for mRNA doses, like Pfizer and Moderna.
Yes that’s meaningless too. The mRNA vaccines are not any more susceptible to evasion than other vaccine types. I’m not aware of any vaccine, including AZ, that doesn’t target the spike protein. Mutations in the spike protein could affect any vaccine.
I thought (from memory) in immunity tests, one specific type induced a far stronger T-Cell learning response whereas the other just mainly blocked the spike? i.e RNA and MRNA are different in the type of protection they provide?
Edit: my memory is good ;)
Loads of year old scientific sudies on the above but this is 2 days old and preceeds B.1.1.1529, for example
I don’t remember that at all. Even if true, it’s not relevant to this discussion.
As to your link, dude:
In fact, he’s claiming that differing hospitalization rates between the U.K. and the rest of Europe suggest that the AZ vaccine may provide longer-lasting protection against severe disease in the elderly than the blockbuster mRNA shots.
Still, Soriot admitted that there was no data to support his claim.
The AZ is an adenovirus vaccine that delivers DNA that makes spike proteins. It’s also going to be less effective if the spike protein gets modified just like the mRNA vaccines will be.
7 months old… only relevant because you questioned it…
The first study to look at the comparative performance of the two vaccines that have been in use in the UK in recent months shows that 93% of people develop antibodies against the coronavirus spike protein by five to six weeks after a single Pfizer jab, and 87% after a single AstraZeneca one.
But the researchers from the UK Coronavirus Immunology Consortium, which includes scientists from 20 different centres, found a difference when it came to the cellular response elicited by the vaccines. That is the generation of T-cells that help fight the virus.
The AstraZeneca vaccine had a greater effect – with 31% of people developing T-cells against the spike protein compared with 12% of those who had the Pfizer jab. People who had the AstraZeneca shot also had a stronger cellular response.
And as I should have guessed, when Churchill doesn’t provide a link to his article it’s for a reason. Turns out it’s an article on an un-peer reviewed preprint that compares a single shot of Pfizer to a single shot of AZ.
So it’s a pre-print on people who literally aren’t fully vaccinated.
You also can’t really measure t-cell immunity well and when the article says there’s a ‘stronger cellular response’, that’s bullshit.