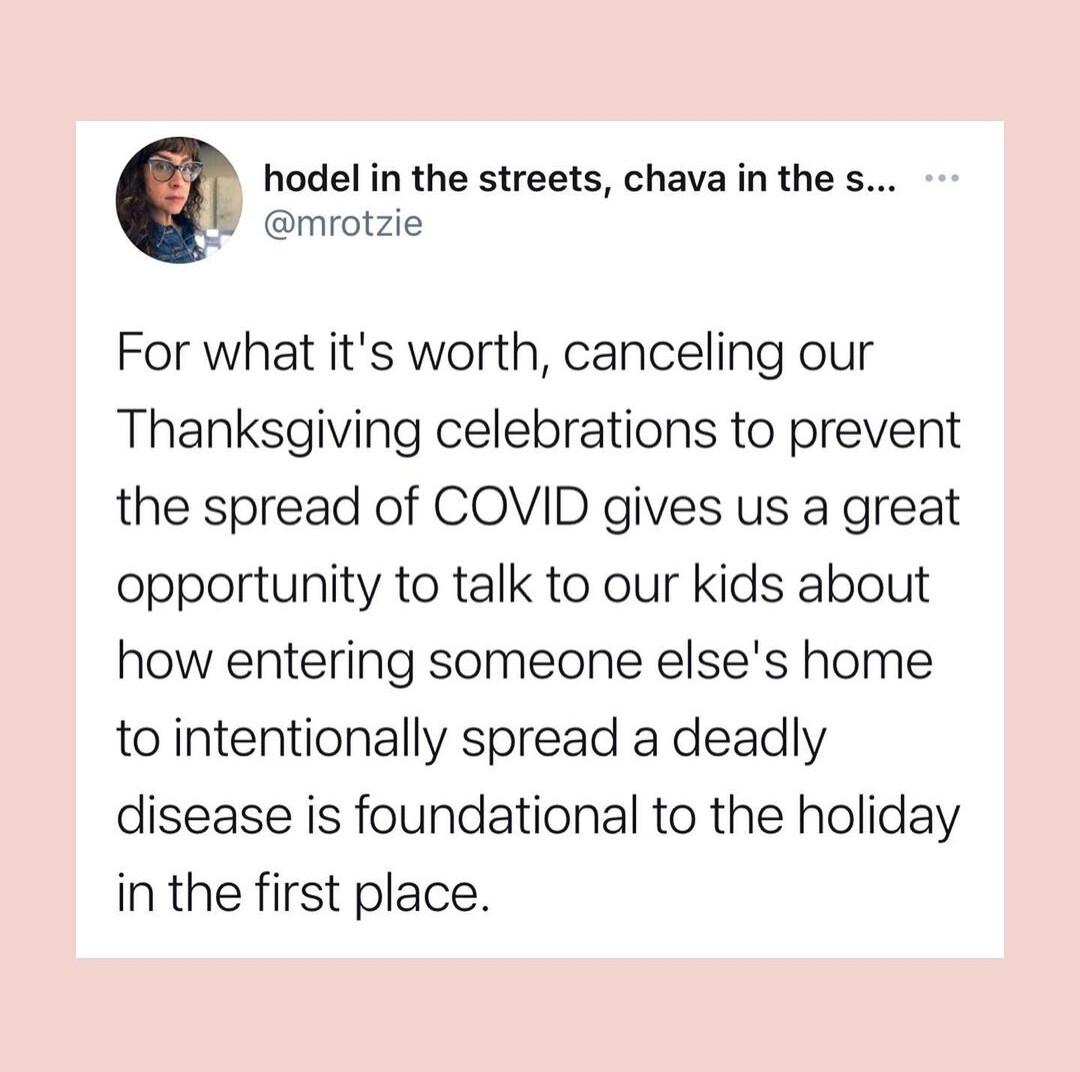
Just read that, and it reads pretty accurate to me. I have a family member currently in the hospital a month after initial covid diagnosis. Hasn’t been intubated yet, but otherwise looks to be at around the nov 12-13 timeline in that thread. I expect there is a decent chance they will be dead in the next week or two. This disease definitely sucks.
…That’s because different doses of the vaccine were mistakenly used in the trial. Some volunteers were given shots half the planned strength, in error. Yet that “wrong” dose turned out to be a winner.
So it turns out someone from work went and picked up there kid from college in a hot spot and broke quarantine rules for the state which would be a fine and our workplace which would be a write up at minimum.
I just got this info after they turned me in for watching tv in the breakroom fifteen minutes after break…what to do…
Sorry to hear that, Jbro. Best wishes for your niece and nephew.
This is the repository that is used for the Johns Hopkins University dashboard. I used it for a while.
So my parents are doing a rapid test tomorrow morning, and a PCR test tomorrow afternoon. They are doing the rapid test because they want to tailgate and go to the OSU game Saturday. Their exposure was Monday.
Can’t remember ever being this frustrated. Fucking. Boomers.
on my way home from work yesterday I thought about going to the bar that my high school friends drink at when they come home for thanksgiving. It was ****ing packed. I didn’t go in because it dawned on me that covid is still a thing.
From chiefsplanet. The Midwest is so fucked. Every day there’s some new story of someone dying or having to go to a hospital 100s of miles away or out of state because their local is full.
The hospital we were just at for the baby is converting anything and everything to rooms. OB rooms, recovery rooms, etc. They are beyond capacity and have people sitting around in the ER waiting on rooms constantly and others being shipped out elsewhere. Not sure where elsewhere is.
Just talked to my sister in Holland. She is a nurse and things are not going well there. During the first wave the hospital was fine but in this second wave there are lots of positive tests in staff and they can’t figure out what changed. So far all her tests have been negative but stress levels are rising fast.
Tell her to quit, imho.
My sister would never quit as to her that would be abandoning her patients and she would never do that. We have lots of nurses in the family and they all think that way. Also means they almost never strike and as a result they have been taken advantage off for decades.
That’s my wife in a nutshell too.
Got my test back, I’m clear, which is absurd, but whatever. I get home yesterday and my mom mentions that some family friends just tested positive and she saw them at some church function. But, she reassured me, we weren’t sitting that close. facepalm
It’s amazing how much of the world’s infrastructure relies on good people putting up with being screwed over. Like the entire NHS runs on this premise.
There’s a huge difference between primary school and secondary school that gets improperly ignored. Older kids are a much better fit for remote learning and more likely to spread disease through non-school activities.
David Greaber talks about this in BS Jobs. There’s an expectation that you will be paid less and treated worse if your job is productive and fulfilling. How dare you have a rewarding job and want more money! You love teaching at a preschool and would do it for free? Ok, be happy with $15k/yr.
TAKE: Time-lagging to determine CFR is a bad idea. Better procedure:
- Go back to the mortality trough in the summer (t0).
- From then until now, add up all cases and all deaths.
- Estimate the number of deaths attributable to cases that were confirmed as of t0. You could probably use hospitalizations times some factor as a good proxy.
- Estimate the number of deaths expected from open cases. Again, hospitalizations can be used to make a guess.
- Subtract 3 and add 4. And you’re done.
The problem with lagging is that you are not really looking for an instantaneous estimate of CFR, so you will end up averaging your daily estimates. And if you average your daily estimates, you are just doing the procedure described above, dropping N days of deaths after t0 and N days of cases up to the present. But rather than spend all your time drawing graphs and eyeballing the CFR from them, why not use it to come up with a better estimate of the tail adjustments rather than the gorilla math of just dropping an arbitrary number of days?