You are starting at a result and working backwards. The data should be neutral.
I’m not saying what the right answer is but the methodology of the economist types is trash.
You are starting at a result and working backwards. The data should be neutral.
I’m not saying what the right answer is but the methodology of the economist types is trash.
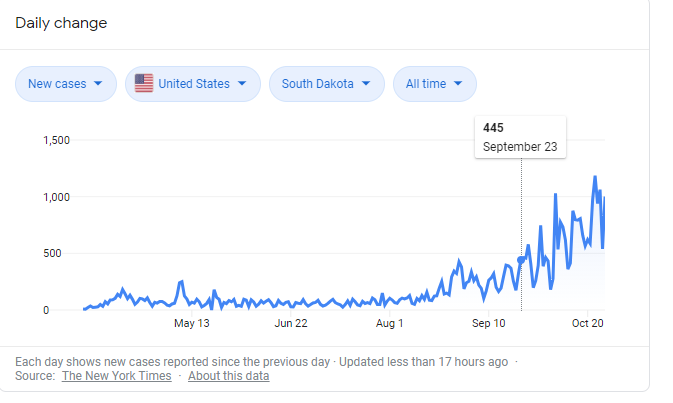
Going to stay on the ND/SD thing. Here’s Steven Millman’s Covid update for August 9th about Sturgis. Here’s the graph for SD. Looks like Steven was off by about a week or so, as numbers started ticking up around Sept 23rd-ish.
August 9th COVID Update: The Sturgis Motorcycle Rally – A Perfect Storm for a Public Health Emergency
Short Version: The Sturgis Motorcycle Rally in SD, due to it’s sheer scale, lack of mitigation measures, and length of stay is likely to kick off a massive public health crisis in South Dakota, possibly by the time it ends. It is highly likely to kick off a new national surge in cases by early September that could last for weeks, followed three weeks later by a new rise in the rate of deaths.
tl;dr – you’d expect nothing less from me at this point. Pull on those chaps and let’s get started. This could end up being one of the worst ideas concocted since the pandemic began.
As you’ve no doubt been seeing in the news, there is a massive event going on in the tiny town of Sturgis, South Dakota, population seven thousand right now. The 80th Annual Sturgis Motorcycle Rally (https://www.sturgismotorcyclerally.com/), running from August 7th to August 16th, may end up being the world’s largest public gathering since the outbreak of the pandemic. Organizers originally expected as many as 800,000 motorcycle enthusiasts to show up but, as with the Trump rally in Tulsa, the pandemic appears to have scared many away. Current estimates suggest that about 250,000 people travelling from all over the country are attending the rally. The organizers made the decision recently that this year, no media passes would be distributed.
You might be thinking, “That’s a lot of people to have crowding into one place while there’s a pandemic with massive community spread going on.” And you’d be right. Events like this represent a near-perfect breeding ground for the virus both in terms of the opportunity to spread the disease, and the opportunity for the disease to be carried to new populations nationally. Much worse is the fact that the event is long enough to spawn two or three generations of the virus and allowing people to get sick before they’ve left the event. This update is focused on what kind of COVID-19 spread we might expect from the Sturgis Motorcycle Rally and what local and national implications might result.
Let’s start, as always, with the numbers and a set of reasonable assumptions. First, let’s use the reported 250,000 as our population estimate for the event. Next, let’s assume that the population coming to the rally in Sturgis is geographically representative of the United States. They won’t be, of course, and there is strong reason to believe that attendees will be more representative of states where the virus is wide-spread. Nevertheless, as always, I prefer to be conservative with assumptions, so let’s go with the attendees being nationally representative. According to Johns Hopkins University, there are about 3.2 million currently confirmed but unresolved cases of COVID-19 in the US out of the over five million total confirmed cases. That, however, is just a slice of the true underlying activity of the disease. CDC Director Robert Redfield recently said that the true number of cases is likely ten times the tested amount (about 32 million) and a recent article in the Journal of the American Medical Association (JAMA Internal Medicine) suggests that the true number of cases is between six and twenty-four times the number of confirmed cases (https://jamanetwork.com/…/jamainter…/fullarticle/2768834). For the sake of this update, we’ll assume the more conservative 10x estimate from the CDC. This means that about 32 million Americans are likely to be current carriers of the disease, or about 10% of the population (that’s a LONG way from herd immunity, so don’t start). Let’s also assume that only about one-tenth of currently infected individuals in the US would be both healthy enough to travel and early enough in the disease progression to be infectious. Taken together, we are therefore assuming a VERY conservative 1% of Sturgis rally-goers, or 2,500 people, will be infected and infectious on day one of the event. Finally, we will use the CDC’s best guess R0 of 2.5 for the degree of infectiousness. The range of R0 estimates has generally between 1.5 and 5.0 in the literature, and once again 2.5 maybe an underestimate of true spread in this population because the motorcyclist population does not include many children and because they will be packed together in concerts, bars, etc. https://www.cdc.gov/…/2019…/hcp/planning-scenarios.html Current reporting across multiple outlets suggests that virtually no one at the event is wearing masks or social distancing.
Remind yourself from time to time while reading the rest of this update, that these assumptions and estimates represent an almost certainly substantial under-estimate of reality.
So. what happens if 2,500 infected and contagious people show up to Sturgis among the 250,000 revelers? The most important reason that this rally is so dangerous is that people will be there for up to 10 days. Not only does this mean that there is time for up to three generations of disease spread, but it means people who arrive sick or get sick at the event will be at the mercy of local public health services that could be come quickly and completely overwhelmed. More on that later.
2,500 people arriving with an R0 of 2.5, will infect an additional 6,250 people within just a few days. Those people will become infectious within the next 2-3 days, a few days before any of them show symptoms (https://wb.md/2WPms48). On day four or five of the event, these newly infected would start infecting others. These 6,250 infected individuals at the R0 of 2.5 infect an additional 15,625 rally-goers. On the last few days of the event people are starting to get sick, and an additional 15,625*2.5=39,062 are infected as they leave the event for home. So, with very conservative estimates of infection and spread, 2,500 infected cases can become more than 60,000 in just ten days, representing about a quarter of all attendees.
That all sounds horrible, of course, but it gets much, much worse from there. If there are 2,500 people who arrive sick, and an additional 6,250 who become infected shortly thereafter, nearly all of those who develop symptoms from that group will do so AT THE EVENT. Most who show symptoms do so around day five, with some sooner and some later. The average age at these events is between 50 and 60 years of age (https://www.blackhillsknowledgenetwork.org/…/aging…), and about 8.2% of those who contract the virus in that age range end up requiring hospitalization. Younger people are much less likely to require hospitalization, and older people are much more likely. For the purposes of these estimates, let’s assume 8.2% as the average. With 8.2% of 8,750 infected, there would be 717 people who will require hospitalizations from among the rally-goers. We are assuming that those infected with generation two or three make it out before symptoms appear, but there’s a good chance that some from the third generation could also require hospitalizations before they leave town. (https://www.usnews.com/…/odds-of-hospitalization-death…)
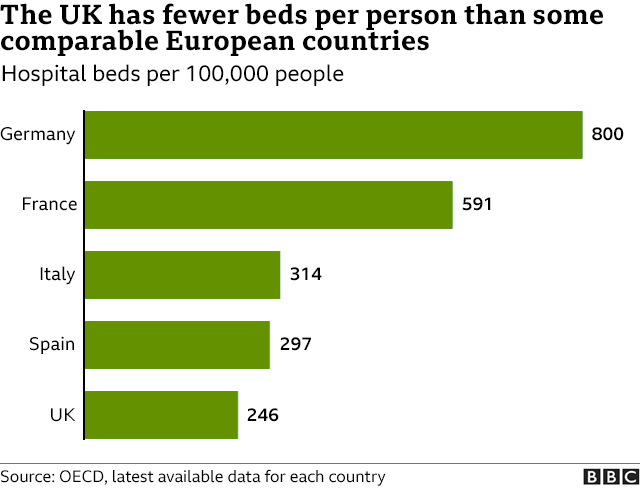
717 people would need hospital beds based on these conservative assumptions. In all of South Dakota, there are only 2,741 staffed beds (https://www.ahd.com/states/hospital_SD.html). This event would require one quarter of the entire state’s capacity. And it’s a big state. Sturgis is in the Southwest corner of the state about an hour from Mt. Rushmore. The closest town of any size is Rapid City, about 30 miles away, which has less than 400 staffed hospital beds. The bulk of the staffed hospital beds (about 1,200) in South Dakota are almost 400 miles away in Sioux Falls. There are no population centers relatively closer than Sioux Falls to Sturgis in bordering Wyoming, Nebraska, Montana, or, North Dakota. The beds are also not all empty. In rural SD (like Rapid City), the typical hospital bed occupancy rate is about 22% and in urban areas (like Sioux Falls), the occupancy rate is about 60%. That leaves about 1,600 empty beds that are available in the entire state, and only about 320 in Rapid City. Less than half of what would be needed. This would be a public health disaster of unprecedented proportion in South Dakota. Not only would this likely increase the mortality rate among the COVID populations, it could create a large amount of incidental deaths among those who need to go to the hospital for other reasons but cannot get a bed or a doctor. In order to manage such a crisis, medical staff would need to be flown in from other parts of the country and sick people will need to be moved elsewhere or to makeshift facilities.
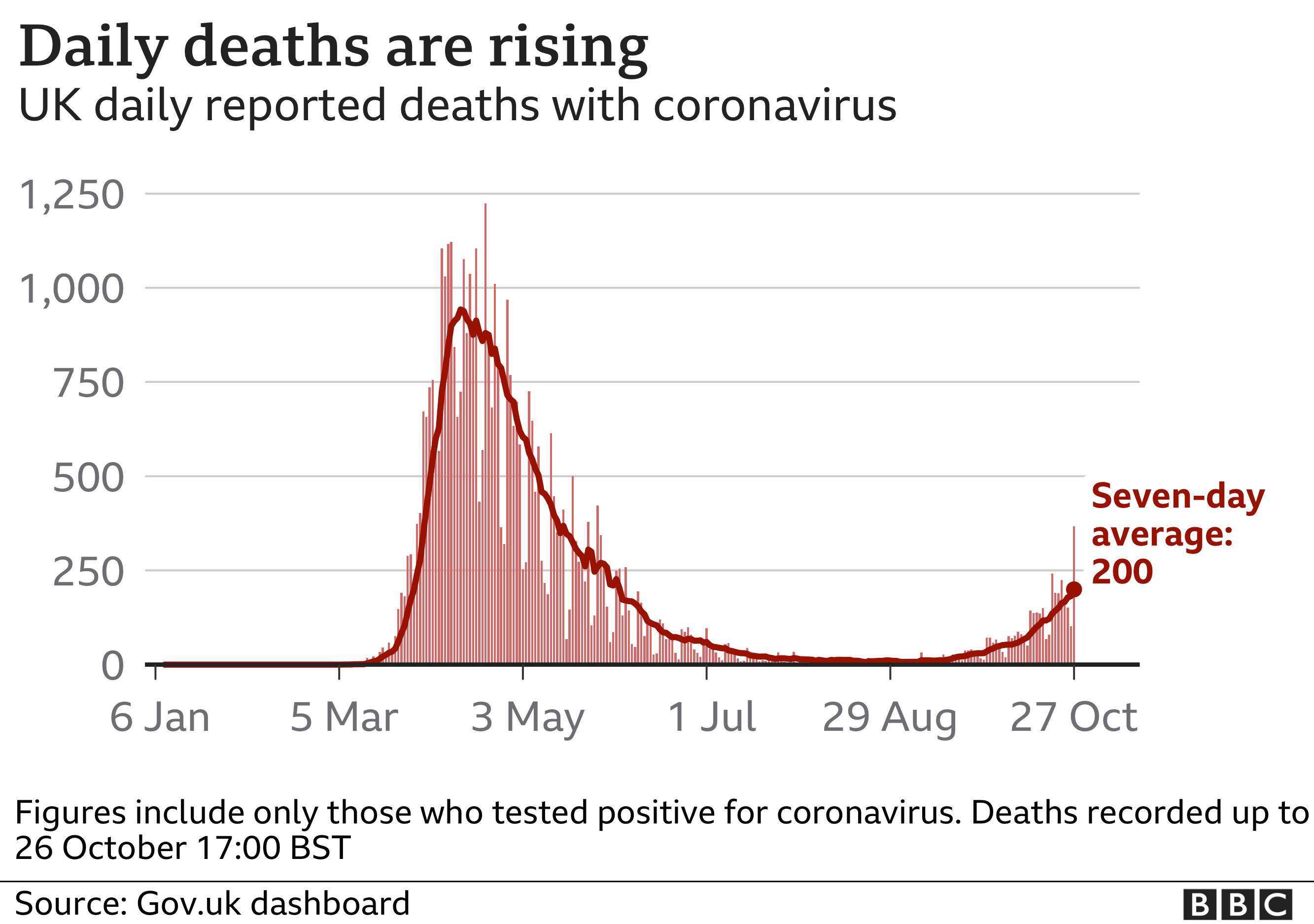
And then there are the 60,000 infected people who return back to the rest of the country, carrying the disease with them. This will show up in the national case data as a bump in cases by mid-September, and could look a lot like the surge we are only now coming out of if mask wearing and social distancing do not improve. Deaths will start to appear as a trend in the National data about three weeks later. Let’s not forget that we’re talking about generally older Americans here who are at much higher risk of death from COVID-19. The average age in the US is about 39 years old, compared to the mid-50’s at the Sturgis rally.
And none of this includes the anticipated rise in community spread of COVID-19 from school openings in areas where the disease is not yet contained. Fall is going to be rough. I’d go into details as to exactly how rough it’s likely to get, but this update is already long enough, and it’s my third update in as many days. I need to take a mental health break (and a whiskey or six), so I’ll do the modeling for expected impacts on mortality from Sturgis and school reopenings in the next update.
I am asking readers who manage to get this far to PLEASE be respectful of the potential upcoming loss of life. I, for one, do not find the jokes about “motorcycles for sale – coming soon” to be very funny. And I laugh at videos of cats knocking kittens down stairs. Imagine.
As always, don’t forget I’m not a medical professional or epidemiologist. I’m a professional statistician with too much on my mind.
Actually, what you said was that we should conclude that school closings are a good idea out of a tribal desire to disagree with economists.
I see now that the point was actually about unspecified methodological disagreements.
France will get put in lockdown again later today, not as strict but that may change, obviously. I’ve not been following the thread and I doubt I’m saying anything that’s news, but all the talk of high cases not being as bad news this time round is demonstrably idiotic.
Yes, France was testing more but when cases rise so, inevitably, do hospitalisations. Maybe the multiplier from cases to people in trouble is bigger, but when you’re dealing with this kind of growth then all that buys is a delay of a few weeks, aka fuck all.
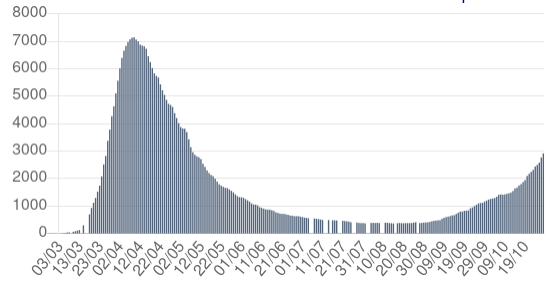
This is France’s intensive care occupancy graph, its ‘limit’ is 5,000. It will in all likelihood be breached before whatever Macron does this evening can have any effect. You in the states are obviously suffering from incompetence and stupidity, but you’re not alone.
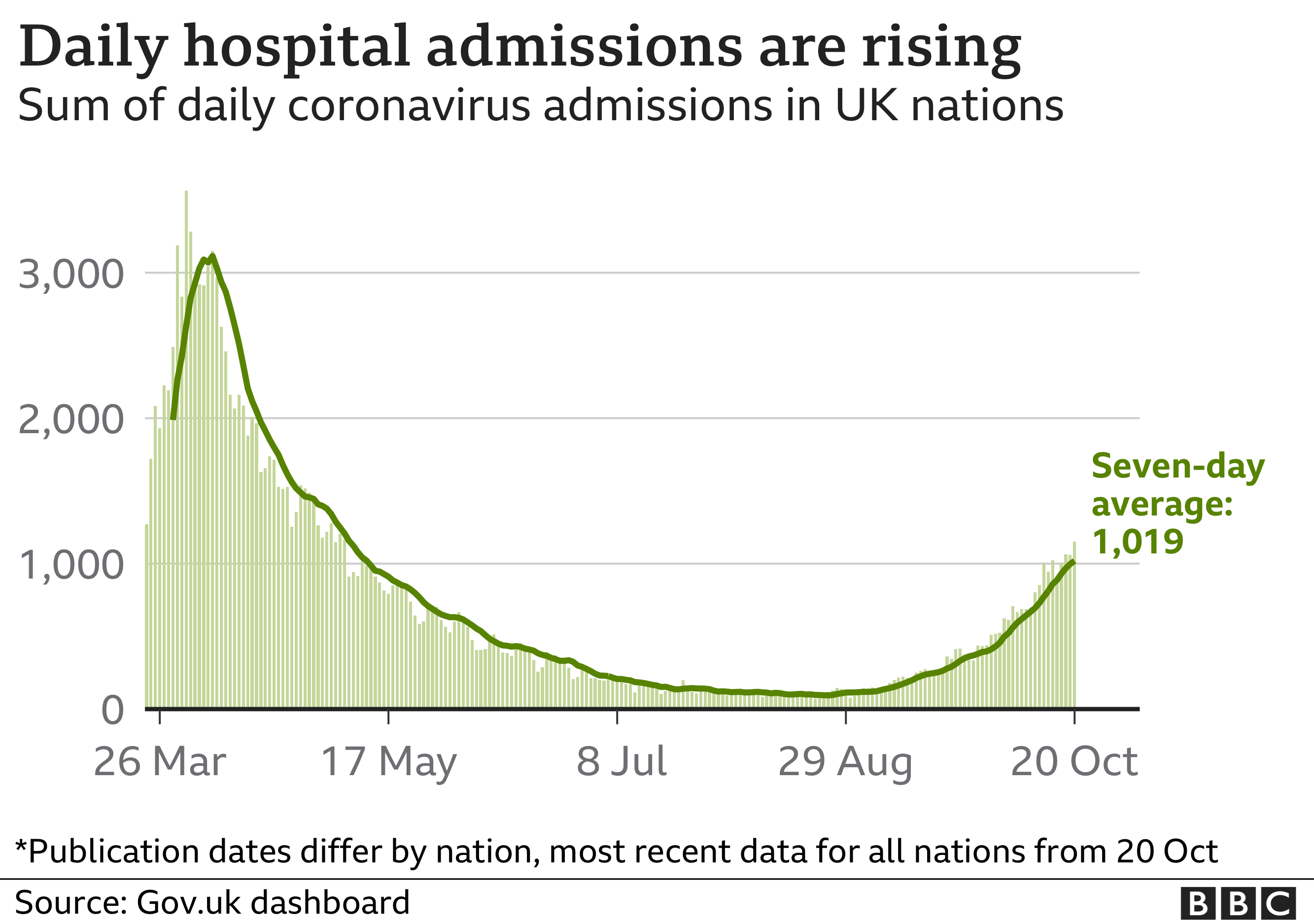
Curve looks similar, although UK’s is deaths…
We’re being told to expect lower total daily deaths, say 600 per day but a US style extended period of said deaths, like 3 months!
Doh!
Just looked at worldometers, US has done about 400k tests per million people. The only euro countries at or above that level are the UK and Belgium. Denmark is at 875k per million but they’re tiny so meh
And Gibraltar, Faeroe Islands, Andorra, Luxemburg, Monaco, Iceland, Channel Islands and Malta - all Europe and above US in testing… and all small so blah
Edited to add Euro test results take 24/48hrs - US test results are like 5 days if you’re lucky, by which time you’ve probably infected others for 2-3 days anyway e.g. Justin Turner above.
So maybe a USA test is ~50% as useful as a Euro test
UK now has a 1hr test for £120 at local pharmacies
compared to size of local outbreaks, usa has done too little, usually after the outbreak rather than during it.
I mean yeah? Sorry I’m not real interested in countries that are smaller than your standard US suburb. Look at the big guys, most are testing at lower rates and if you look at Europe as a whole they’re testing about 285k per million people
i think there’s probably something to testing low totals if locality doesn’t have a high rate of community spread, and locality has effective contact tracing. smaller countries probably do a much better job at those than 50 different governors and some mayors.
It’s hard to compare testing across countries as they have different definitions of ‘a test’ and the continent and country you compare use different tests. If you remember back 9 months, the US didn’t pay up for the WHO test and devised their own, which was wildly inaccurate so bought a plane load from S Korea. EU use the WHO test.
Does each US state count ‘test’ and 'death’in the same way? Also comparing US to a continent, you need to factor in Canada’s test when comparing continents - might drop North Amercia lower again
The number of people tested
The number of tests is not the same as the number of people tested. For clinical reasons, some people are tested more than once. Therefore, the number of tests will be higher than the number of people tested.
There are several valid reasons why some individuals may be tested more than once, including:
- regular testing of health and care workers
- individuals who have the virus, test positive, and have a subsequent test to see if they can return to work
- participation in early trials comparing healthcare professionals administered tests with self-administered tests, resulting in two results on the same day
- participation in research studies conducting routine tests on the same people each month
- some tests may come back as ‘void’ and a retest would be issued
- individuals with early symptoms who test negative, develop more symptoms and are retested and found to be positive
People tested figures are published as part of the weekly Test and Trace publication. Many people are retested multiple times for valid reasons, such as regular testing of health and care workers over several months.
The ‘people tested’ measure was initially used to avoid counting one person tested several times in a short space of time. It does not reflect the volume of tests carried out each week, especially given the importance of regularly testing workers in social care settings. We’re publishing tests processed which shows the number of tests we have results for.
I suspect this info isn’t published in the US
Of course it was. Nobody would ever willingly travel to North Dakota, so they were essentially an island prior to Sturgis
Only the fucking Dodgers could turn “First championship in 32 years*” headlines into “Look at these dumb motherfuckers willingly allowing their Covid positive player to infect everyone around him” hesdlines
Belguim has 11 million people so that’s a big suburb. But i get your point.
Also a lot of those test are coming from the northeast. If we take the median state and compare per capita test I dont think we are doing much better.
Without looking I can say for sure that New York is a huge percentage of overall US test relative to population
I mean compare New York to FL TX AZ. And the difference is huge. And I dont think places like FL or TX have the ability to scale up in a crunch IMO.
China? Tested a city of 9m population in 5 days last week. This week the next city to be tested was 4.8m population because of 1 (one) covid case traced
China’s one country like US - but hey, Worldometers (.com) not including their testing rate, DUCY
So Germany goes back to a partial lockdown for November. Schools stay open. Barbers too. Pretty much everything else closes like restaurants, massage salons, swimming pools etc… Churches are allowed to stay open. That will probably sending some lawnmowers into orbit. I assume the government is afraid of their lobby.
A broad but limited German lockdown will now start on Monday 2 November, under terms agreed during a video conference involving Mrs Merkel and the 16 state premiers:
- Schools and kindergartens will remain open
- Social contacts will be limited to two households with a maximum of 10 people and tourism will be halted
- Bars will close and restaurants will be limited to takeaways
- Tattoo and massage parlours will shut
- Smaller companies badly hit by the lockdown will be reimbursed with up to 75% of their November 2019 takings
- Mrs Merkel and the state premiers are expected to reconvene on 11 November to reassess the situation
I can’t find it now but there was a twitter thread on Monday that takes down the NYTimes articles use of data point by point.
Essentially the economist/writer cherry picked the euro data too early and that as time has gone on its looked less and less favorable.
Also the writer today was pointing out there is a big difference than your private prep school environment and either inner big city school or your small town rural red state without mask mandates.
My point is garbage in garbage out. I deal with microbiology data on a daily basis. You can literally find any correlation you want. But if it’s not founded in the fundamental principles then the bar for accepting your conclusions is much much higher.
Sometimes you discover something new so you can’t be closed to novel conclusions and hypotheses but when the math says 2+2=5 you better go the extra mile to make sure there isn’t something lacking in the data, the maths, or your logic.
I personally think we can open some things with good masking and social D if we have priorities. But that is not what is happening. Let’s party at bars and indoor dining and sports locker rooms and then let’s open schools.
When you prioritize everything you prioritize NOTHING.
And yes I’m very suspicious of economists at this point. Most of the bullshit data mining is coming from them and they make the most hate brained assumptions about biology and get it wrong seemingly every time.
Regarding the data folk vs the epi folk.
There’s been less than ideal takes (and interpretations) from both camps pretty consistently throughout.
But it gets magnified into bad takes once the analysis gets translated into digestible population level messaging.
Then it just gets ridiculous once caveats are removed for brevity and any lack of nuance is stripped into click-bait style twitter quips.
Like, I’m a data guy but I’ll gladly defer to the epi sources. Buts it’s got to be first source AND its got be simple enough for my caveman brain to comprehend.
Oster’s point is likely undeniably true. ~in areas with very low transmission; its better to have elementary school open and prioritize that over bars.
Like duh, but that is so far from “let her rip, kids don’t get it” and especially when the data used to make the claim are 2 data points from suspect samples (that lol, dont even support the claim!!)
On the epi side, an example is the IHME model. It got a lot of flack but its not an unreasonable forecast given the caveats they had in place. But then taken without the caveats and the wide margins of variability built in, you get lol single digit prognostications and subsequent denunciations.