The more accurate and direct response to me would have been:
“I believe that High SDI leads to lower cases and Low SDI leads to more cases. I also believe that testing data has been unreliable for several months. I don’t actually have strong evidence that any of this is true, but I still believe it. I’m not a scientist, am not a skilled data analyst, and I’m not interested in trying to prove to someone else that my beliefs are true.”
I woudn’t have any issue with that response - you don’t owe me (or anyone else) any kind of evidence. There’s no shame in not being a scientist or being a data analyst. I don’t know how to play the piano, and I’m not a very good swimmer. But it’s a fact that absolutely nothing you’ve shown represents any kind of objective, falsifiable evidence to support your beliefs. So I’m going to continue to dismiss the SDI discussions and graphs until/unless someone can point to evidence that they’re meaningful.
As for this:
I look forward to seeing your cite to me downplaying the pandemic.
I do remember being more optimistic than some other people on here, saying things like:
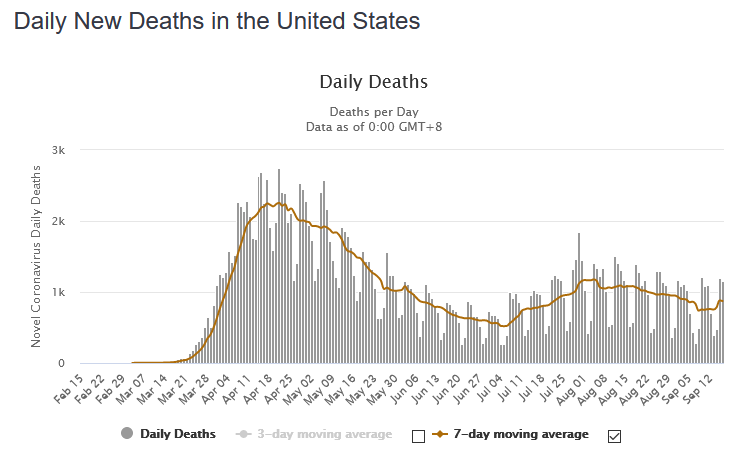
- Deaths in August were going to much closer to 2k than 3k (to someone who thought 3k was inevitable)
- Average daily deaths in August were unlikely to exceed 1.5k
- “My estimate for the peak is that the highest 7-day average deaths will be between 1,350-1,790 and will be somewhere around the 7 days from 8/2-8/8.”
Those were all in July and I feel pretty ok with them based on how things have gone since then:
But again, I look forward to seeing your evidence of me downplaying things.