EDM?
We’ve known and talked about the excess deaths showing how much covid is undercounted for months. I wouldn’t be surprised to see it go up above 30% with all the red states getting deaths now, as they are likely to undercount by even more, but I’m not assuming that until the numbers show it.
I’m up for masking up during flu season.
I don’t disagree with this in general. But Do try to be conservative for now.
I do think the case of population A where it gets straight into old folks home and population B where the initial wave is bar hopping young people will have A>>B. A is kind of everything goes bad- old people, overloaded systems etc.
Ah when you google “nyc covid deaths” it gives you the state numbers. Still 0.28% makes 0.5% a fantasy unless something drastically changes in treatment. It’s also too low.
1 Like
Modular synthesis. This guy was a conductor for London Symphony Orchestra and now just does modular mostly. My machine is not near as big as his. I also mix VCV Rack software and he does all hardware.
3 Likes
It’s already in my previous post, sorry if it was unclear. The 3 charts were:
- Weekly Scaled SDI vs Scaled Cumulative Cases
- Weekly Scaled SDI vs Scaled New Cases
- Weekly SDI vs New Cases (Scaled y-axes rather than scaled data)
What I was trying to get at is #2 and #3 are visually identical but #3 is better as it retains the unit context for both y axes.
“ What is herd immunity, and could it play a role in stopping the spread of COVID-19?
Herd immunity occurs when enough people become immune to a disease to make its spread unlikely. As a result, the entire community is protected, even those who are not themselves immune. Herd immunity is usually achieved through vaccination, but it can also occur through natural infection.
Based on what we know about the contagiousness of the COVID-19 virus, experts estimate that somewhere between 60% and 70% of the population needs to be immune in order to achieve herd immunity. That’s close to 200 million people in the United States, and nearly five billion people worldwide. (As of now, we are nowhere close to the numbers needed to achieve herd immunity.)
Achieving herd immunity through natural infection means many people would become ill and many would die. These risks may fall as we develop effective treatments. However, we still don’t know how long people who recover from COVID-19 will remain immune to reinfection.
Ideally, we will achieve herd immunity through a safe vaccine (or vaccines) that will confer lasting immunity.”
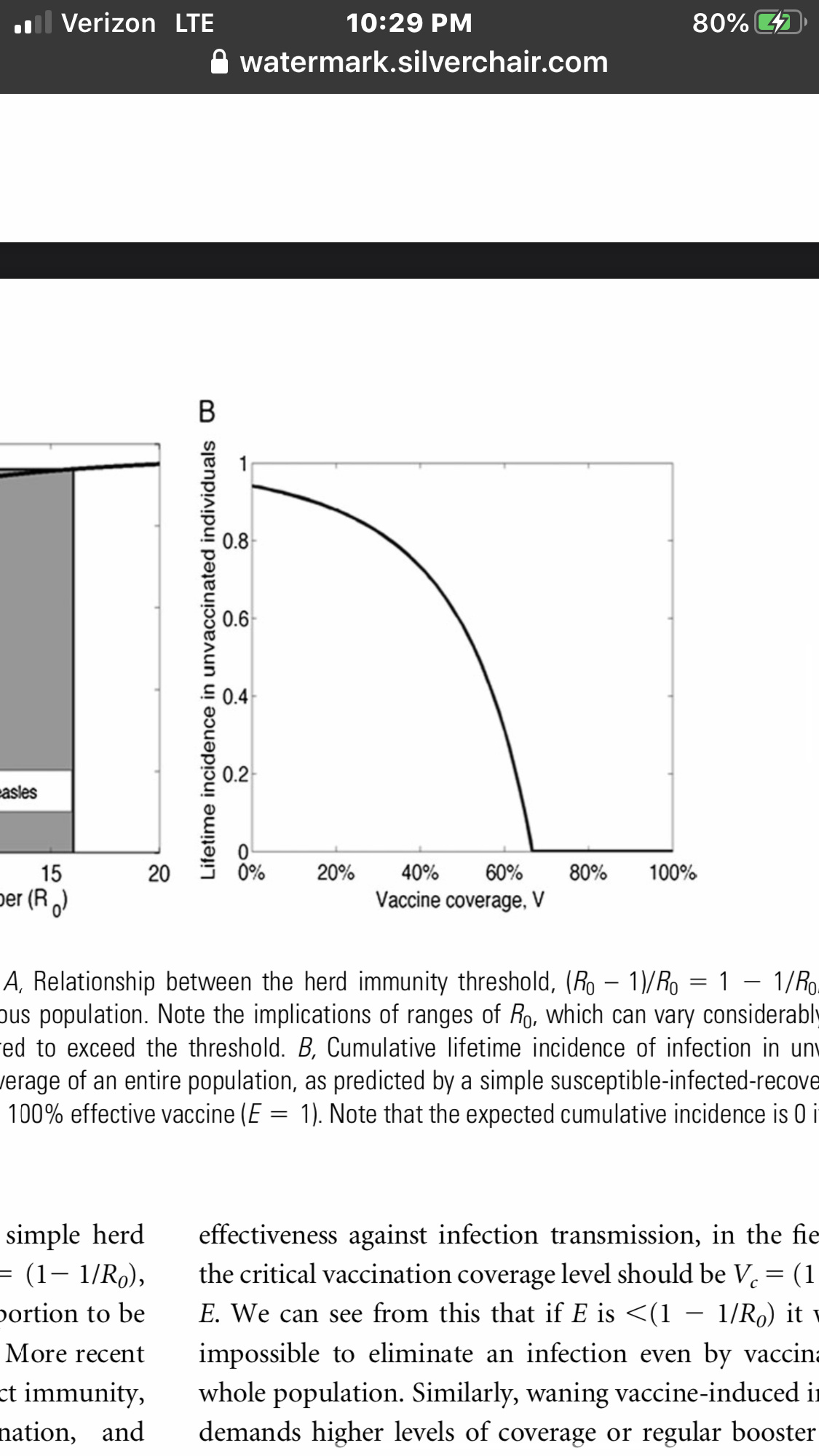
I read this is that the majority of the protection kicks in at the high end. At 20% you aren’t getting much protection at all.
1 Like
Tap. Tap. Is this thing on?
Again, I never said NYC was .5%. Obviously it was around 1%. Spain and Italy might have been even higher.
Yeah, it looks like I’m doing something pretty similar with my SDI graphs. I just try to make the numbers not smash on top of each other when I’m resizing them. Thanks for trying.
Please read this: How Herd Immunity Happens - The Atlantic
Mainly the second half about behavior changes. The heterogeneity stuff is speculative. 60-70% herd immunity assumes a population essentially doing nothing to stop the spread.
20% can get you a lot if over 50% of the population is isolating and wearing masks and continues to do so. It doesn’t mean the virus isn’t waiting for its chance to get into that fertile ground (IE - sending kids back to school). But if it doesn’t get it’s chance, 20% could turn into a slow burn for a while.
I’m probably not going to get covid. My Dad is even more scared than me, as is my boss and a bunch of other people I know. So you can remove us from the pool - at least for the near term - which is what this whole discussion was about. How many others like us can you remove from the pool?
I’m not saying this is enough herd immunity to kill covid. I don’t think it is. But it could be enough to keep the fall from blowing up - which is how all this started.
It was more than 1%. There’s an additional 5k excess mortality deaths in NYC. Again, 0.5% is very optimistic at best. 0.7% and you start getting closer to reasonability. Sorry if that makes you mad.
It’s very possible some amount of thumb on the scale - but we have no reason to think those states weren’t doing that before as well. We also know that all those states did implement various shutdowns and SDI measures in hotspots.
@nunnehi. I think you might be able to bracket your SDI. Let’s go with 5
Let say at target SDI we use a daily case multiplier of 1.00.
The rang directly above and below give some adder or subtracter of lets guesstimate 0.03. So if we are below SDI by some value (5-10?) then cases grow at 3% a day. (Or shrink by 3% on the good side)
Then anything outside those ranges we use 1.05 or 1.06.
(You May want to use 1.x^7 to represent weekly change)
Could you then see how week prior weekly SDI predict the next weeks growth (next week to account for the testing lag).
(I want to stay away from R0 due to all the various way it is calculated).
Make sense or am I babbbling after a 10 hour drive.
Thanks for the info
I think cfr is above 2% based on cfr all over the world and in the US other than places that are exploding (so denominator is going up much faster than numerator right now)
Why is .5% optimistic at best? For what kind of population? What if your population was all teenagers and pro athletes? Still .5%?
I get that because NYC had 1% or more that makes it obvious to you that .5% is wildly optimistic for any population - to the point you don’t need to back it up with numbers. But I’m not buying it unless you make an actual argument.
IFR of NYC caught flatfooted in March is not guaranteed to be anywhere close to Florida with olds/at-risk largely isolating and youngs out there partying it up in July. Just think of what one nursing home blowup does to your IFR. NYC had dozens of them.
Yes I know there are examples of stupid olds in FL not isolating. That doesn’t mean a significant % of them are out there being idiots or still thinking it’s a complete hoax. Even the right-winger olds I know seem to be taking it seriously by now.
NYC is one of the healthier areas of the country (google the stroke belt if you’re interested) with better access to care than other parts of the country. While treatments are improved and hospitals were overwhelmed, it is extremely unlikely that accounts for what would be a massive difference in IFR.
The only way you get to IFR of 0.5% is if steroids/anticoagulation have massive benefits, the initial surge to NYC hospitals is what killed a ton of people, and there’s a large enough population shift in who gets exposed. I suppose it could happen, but you need a lot of things to go right.
1 Like
Totally agree that it’s higher or lower depending on population age, risk factors, etc.
But general population 1% is a good range.
Breitbart and what has to be bots are pushing… wait for it…
hydroxychloroquine…
Is that the best they can do?