A. I’m really tired and today’s discussion is a lot to digest
B. There are a lot of unknowables here. Try not to get too personally vested in any number.
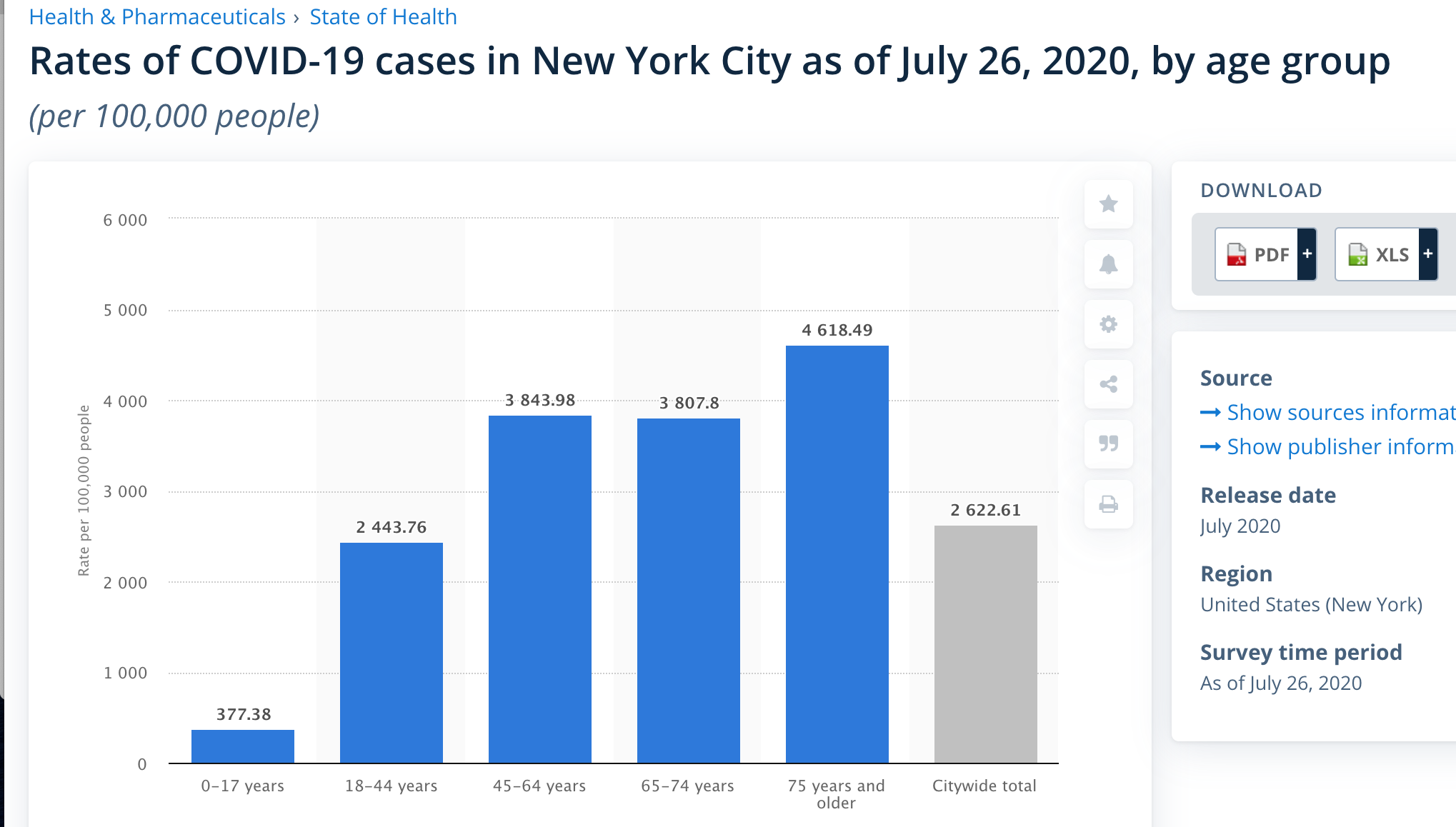
C. 0.5 is the bottom number. The NYC data is good case in point. If the purpose is to forecast deaths it’s a good bottom range estimate. I’d use 1.0 has the high end. But as I stated before CFR is the actual available number, even with all its warts.
D. I’m sure that behavior shifts herd immunity from the standpoint of lowering the transmission rate. I just assume that the shift is mostly the behavior and very little the antibodies. Look at countries around the world. The best performers are all behavior based. Many of the poor performers immediately start going back up as soon as they relax the good behavior. I don’t have the math to back it up. I do think it’s fair to say that behavior>>antibodies in the population based on observed results. maybe the spike rates are somewhat shallower but that’s it for the under 20% immunity range.
E. We can know and can’t trust the antibody effect for now. So it basically changes nothing. Focus 100% on behavior.
F. At high case density it WILL get the old people. Any hope otherwise is just thoughts and prayers.
G. Get the background low then continue good behaviors. Wear a fucking mask. Don’t have crowds. No estimates here change this.
H. Take a day off if you are getting offended. Dealing with unknowns sucks. Concur with Bring your receipts- show your math/logic.
I. Good night. I got to read my grandson a bedtime story tonight after an 8.5 month interval. Focus on something positive.
FWIW this analysis is looking high at the moment. I’m not sure if we’re getting to 2000 confirmed deaths/day, at least in the next 3 weeks. Spidercrab’s 1500/day peak of this wave feels about right.
Florida’s CFR+28 looks crazy low for whatever reason. If they were maxed out on tests the CFR should be higher, not lower. Assuming people usually get tested before they die.
It certainly makes you wonder if a much younger population is getting infected right now - in addition to whatever shenanigans FL is pulling.
Bronx and Queens were hit the hardest - they have a lot of the same health problems that are hitting latino and black communities very hard right now. Manhattan and Brooklyn got it the least.
This has some stuff about the demographics of the current wave:
In Florida, where the coronavirus has infected more than 311,000 residents, the median age of positive cases in March was 65. As of July 17, the median age of new cases from the previous 14 days was 39.5.
Nationwide, “the average age of people getting infected is now a decade and a half younger than it was a few months ago,” Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, said in a July 6 press briefing.
So is the dispute here that one side says a random person getting infected has about a 1% chance of dying, but Suzzer is saying that of the people getting infected today, a random person in that population has a .5% chance of dying? Trying to parse out the situation here.
It won’t change it enough and using the nyc data like that is very flawed because you had to be hospitalized to have a decent shot at getting a test for a long time
In The Bronx, which has long grappled with lower-than-average life expectancy and high incidence of chronic health conditions like asthma and diabetes, those infected with coronavirus die at a rate three times higher than those who live just a river away in Manhattan.
Florida is very big and diverse. It’s not all going to have the same profile as the Bronx or Queens.
The Bronx being less healthy than the rest of New York isn’t contradicting me when I say NYC is healthier than huge parts of America, especially the south.
Then show your work for once. Show Florida and convince me it has the same profile as the Bronx. It’s a big diverse state. A lot of younger people move them from other places - like Manhattan.
Show that a median age range of 38 is going to barely affect IFR.
You just keep asserting things and I’m doing all the work posting actual links and arguments.
Believe it or not I’m not especially inclined to do a bunch of work for someone asserting that I said median ages of a population would make no difference. Or in general really. Cheers