Eh, it’s in human nature to prepare for the worst in an unknown situation. This virus has a way of surprising everyone. I approach everything COVID-related with the understanding that there’s a great deal of uncertainty on either side. If this actually does spread better in the winter we could be turbofucked. Or it could gradually peter out, no one knows.
My mom is skeptical that we’ll ever have a working vaccine against a coronavirus because we’ve never done this before. From what I’ve read, we were pretty close to having a vaccine against SARS and MERS but they went away on their own and research stopped. She’s still not convinced, which has me a little worried.
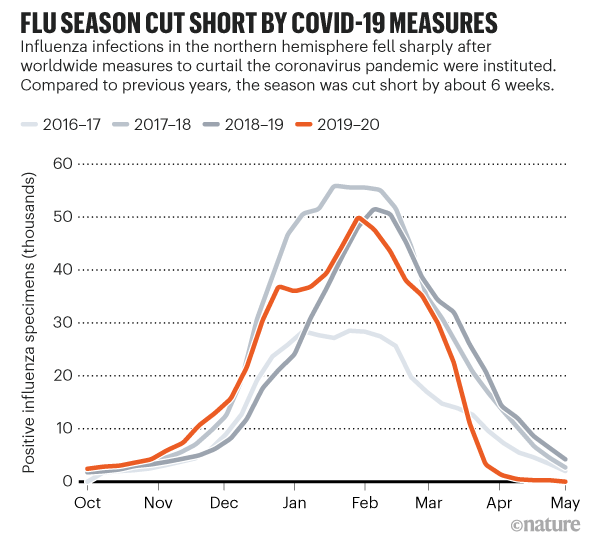
Sucks for the flu, though, right? Flu deaths are way, way down this year. Flu was just minding its business doing its thing when everyone started socially isolating and wearing facemasks. Like, what the fuck?
I said a team that just got 3 positive cases in the past 2 days will have 10 total (so 7 more) within a week. These players played the game with others in the dugout etc not social distancing and who knows what in locker room and hotel room.
Yeah I think about if no vaccine works a lot. People are counting on it and it’s still a huge wildcard.
Sometimes I’m the optimist in the room. Sometimes I’m the pessimist. On this site I tend to be the optimist more often than pessimist obviously.
My only two goals are to filter out the noise and figure out how to keep me and my loved ones safe, and figure out what to do with my nest egg. So I have no other agenda.
This makes no sense. You calculate IFR by testing people and seeing how many die. If an untested person dies it should not affect the IFR calculation regardless of whether they had it.
But anyway, the stooopid scientists know what they’re doing more or less and they’re spending a lot of time working on it. Whether it’s the awful, corrupt CDC or the WHO or whoever, you can’t just “add 30%” because of something you just thought of.
The numbers are predicting 7DMA for each week until 8/17. USA totals at the bottom.
I centered the 7DMA over the middle of the week (because I used a centered 7DMA to get my original 5% CFR that this is based on), so 10 days from the starting point.
The basic formula is I looked backwards to get a CFR (-1 month) of 5% for the 3 states with 20% positivity rates. So I normalized 5% CFR to 20% positivity then bumped it down or up from there. So 10% positivity = 2.5% CFR. I also did a version where I set a floor of 2% CFR - which added about 100 deaths per day at the end.
Oh yeah to get the numbers in the middle I just took the difference of predicted deaths and current deaths and divided by 4 - very scientific.
Yeah, but you still have to know if someone was infected. CFR is higher because of the way you find out if someone was infected or not. The difference is you need to study and test a whole population prospectively or do random sampling, not base it on tests of people who might just be getting tested because they have symptoms.
Unless you go back and test them later. IFR by definition includes untested people. CFR does not. Estimating how many untested people had it is the tricky part.
IFR over that general population is at least 0.6% (that would be at 50/50 and it wasn’t)
I agree that young people are waaaay below 0.5 IFR
There are 50M Americans over 65
We have a lot of deaths to go given how dumb America is acting about this.
If people on this site don’t think there will be that many deaths or that high a death rate then joe public is never going to so we will continue to do dumb stuff. Thus I get frustrated when people on here downplay what is happening.
You can estimate infection rates and IFR by looking at deaths overall and eliminating other causes, I guess, but you have to have a way to get at the number of people infected…and then see the rate at which they die. What we’d like is something like a big random sample of the population tested and then for them to be followed.
I know “it’s just like the flu!” is an annoying right-wing meme, but what if we all decided to treat the flu as though it was a serious disease that kills 20-60 thousand people a year in the US and hospitalizes god knows how many people? OK, forget about deaths, it’s just bad for business when people call in sick, right?
Imagine if we all got a flu vaccine, and if Amazon warehouse employees could take sick leave if they developed flu symptoms, and if wearing a mask because fashionable during flu season. That guy you work with who shows up to work sick as a dog, imagine if that kind of behavior was deeply stigmatized.
We could legit have a chance at stopping some of these endemic viruses.
To guess at current IFR - you basically have to assume confirmed cases to actual cases ratio based on previous studies. Or to get current actual/confirmed you assume an IFR based on previous studies. So it’s a little of a Catch 22.
And of course you know the problem is those numbers are always in dynamic flux. IFR fluctuates with population and treatments. Actual/Confirmed cases fluctuates with testing availability and severity of infection among the infected population.
Unless there’s some other way to triangulate on these numbers like hospitalization or something I’m not thinking about. @Danspartan?
What we need is a new massive swab study in the US now encompassing a whole area.
I don’t want to fight about predictions, because we don’t know what’s going to happen. But I want to lay out my very simple math to try to understand what’s causing you to come up with such different numbers.
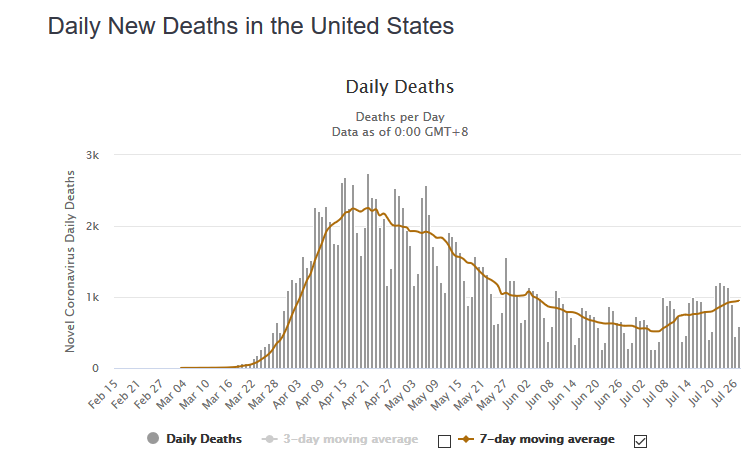
Basic algebra is that average daily deaths for a given period ~= daily cases from an earlier period multiplied by the average CFR for those cases.
Looking at aggregate U.S. data from covidtracking.com, we have roughly 68k average new cases, with a recent apparent plateau:
(Of course testing limitations put an artificial cap on that number, but those same testing limitations will inflate the estimated CFR because they reduce the denominator.)
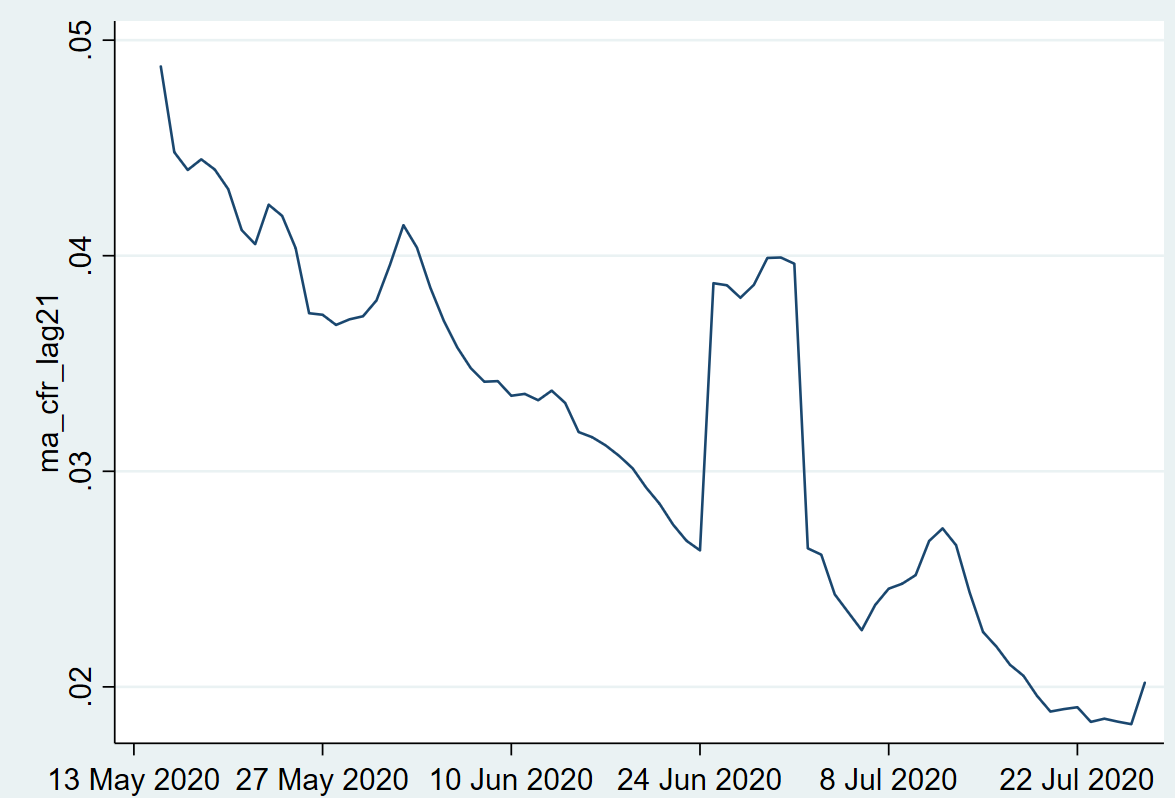
As far as the expected CFR for that cohort goes, using 7day average deaths over 21-day lagged average cases, I get about 2%:
So this is where the 1,200-1,400 number comes from in terms of expected future deaths: around 68k cases * 1.8-2% CFR for those cases. (That’s a 7-day average number.)
I have no idea where your 1,500 daily number is coming from. (I assume that’s a big prior data dump that I haven’t seen yet.)
But my view is this: If you’re expecting a significant increase to 1,500 average deaths a day or more, it means either a huge increase in reported positives (with a constant CFR for that cohort) or a huge increase in CFR (for a constant level of positives). Both are possible, I guess, but I’m puzzled by your certainty that one or both will happen. What makes you so sure that we’re going back to mid-May # of average daily deaths? That seems like a really aggressive assumption, and I’m not sure why my “things will probably continue roughly like they have been” prediction is delusional.
I dunno man, I see you always making the rosiest predictions out of hope and then naysayers here saying otherwise. The recurring heat theme is not something to fall back on though imo. I’ve been wrong a lot of times though.