The new analysis — by Mandeep Mehra, a Harvard Medical School professor and physician at Brigham and Women’s Hospital, and colleagues at other institutions — included patients with a positive laboratory test for covid-19 who were hospitalized between Dec. 20, 2019, and April 14, 2020, at 671 medical centers worldwide. The mean age was 54 years, and 53 percent were men. Those who were on mechanical ventilators or who received remdesivir, an antiviral drug made by Gilead Sciences that has shown promise in decreasing recovery times, were excluded.
Mehra said in an interview that the widespread use of antimalarials for covid-19 patients was based on the idea of “a desperate disease demands desperate measures," but that we have learned a hard lesson from the experience about the importance of first doing no harm.
In retrospect, Mehra said, using the drugs without systematic testing was “unwise.”
“I wish we had had this information at the outset,” he said, “as there has potentially been harm to patients.”
Nearly 15,000 of the 96,000 patients in the analysis were treated with hydroxychloroquine or chloroquine alone or in combination with a type of antibiotics known as a macrolide, such as azithromycin or clarithromycin, within 48 hours of their diagnosis.
The difference between patients who received the antimalarials and those who did not was striking.
For those given hydroxychloroquine, there was a 34 percent increase in risk of mortality and a 137 percent increased risk of a serious heart arrhythmias. For those receiving hydroxychloroquine and an antibiotic — the cocktail endorsed by Trump — there was a 45 percent increased risk of death and a 411 percent increased risk of serious heart arrhythmias.
Those given chloroquine had a 37 percent increased risk of death and a 256 percent increased risk of serious heart arrhythmias. For those taking chloroquine and an antibiotic, there was a 37 percent increased risk of death and a 301 percent increased risk of serious heart arrhythmias.
I celebrated Open For Business today by getting fast food for the first time since early March. The woman at the money window had her mask below her nose. The woman who handed me my food had her mask on her chin. Guess I’m back to sandwiches at home for the foreseeable future.
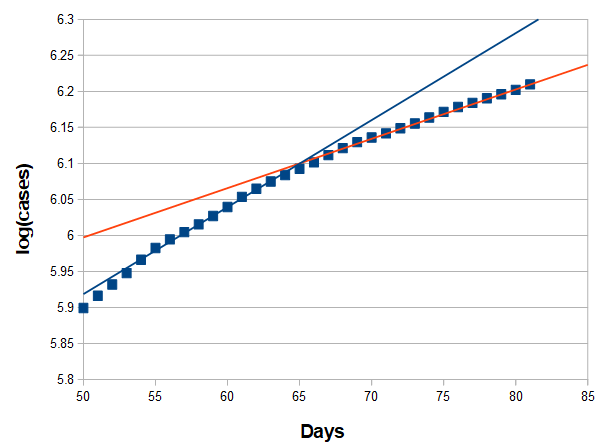
Last few days the rate has been pretty constant as decreases in NYC and elsewhere balance out growth elsewhere. Still lower than when the lockdowns started lifting. Thing to look for is if the orange line starts to trend back up.
Right now, we’re on track to hit 2 million cases in ~2.5 weeks.
Epidemiologists in Europe stated that the virus has adapted differently in each country and that travelling over the summer will mix the strands together, thus making things more difficult for us to deal with.
It’s just more likely to happen (a mutant arising). Better or worse is impossible to say. I do think some of the factors that favor a weakening are absent in this thing. It already doesn’t kill its victims off too fast. Spreading more efficiently is favored. Damage to the host is essentially neutral to the virus.
And remember. Mutations happen all the time. Then selection and chance determines if a particular mutant thrives.
What source are you using for this? I’ve been using the states dept of health site for tracking and it always takes a few days for each days case numbers to fully update. According to their data MN high was May 4 with 819 cases.