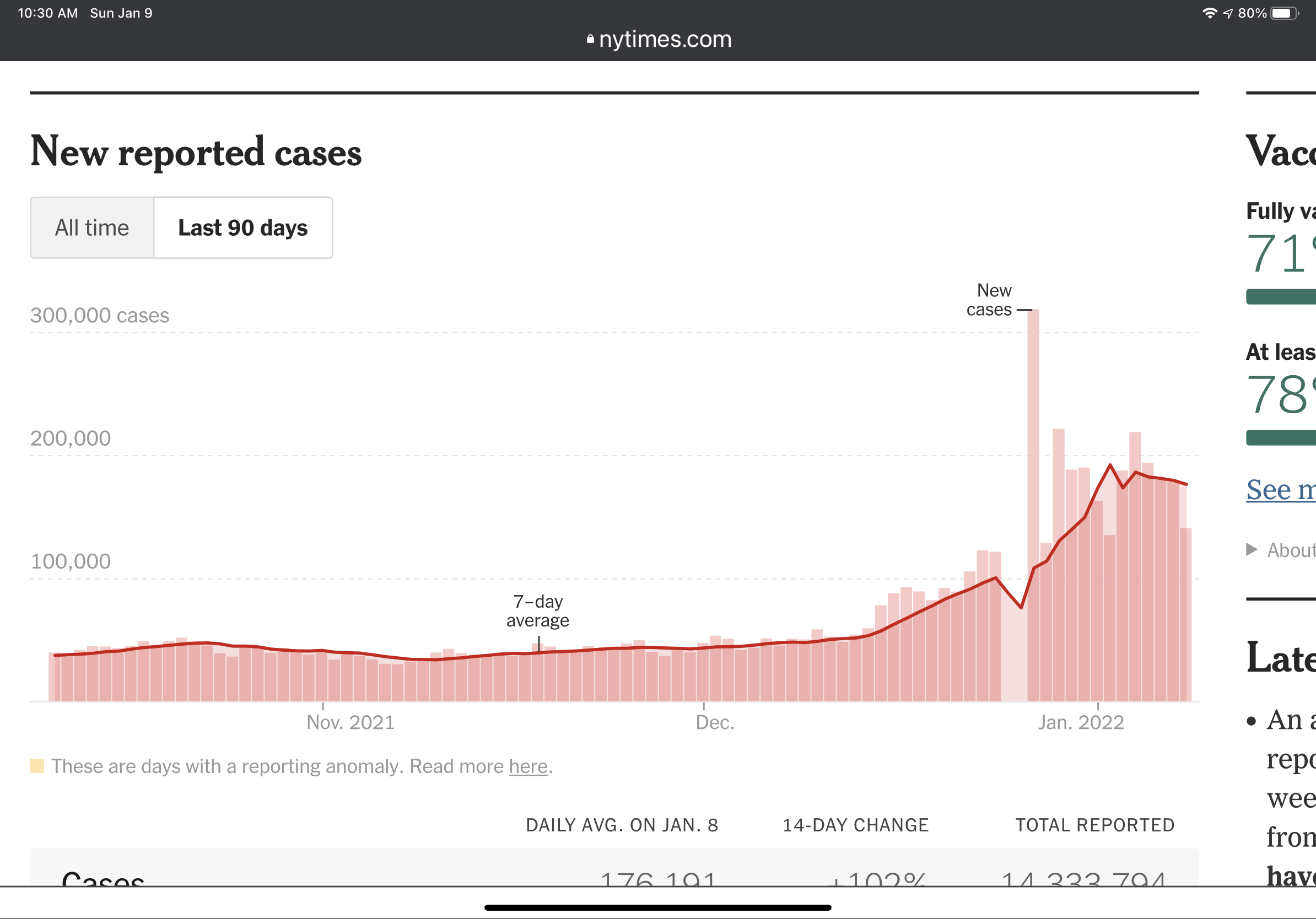
We also don’t have a comparison to prior waves and variants. So the number in isolation…I’m not sure what we make of it. Also, I haven’t looked at the data, but eyeballing that chart by region, I feel like there might be some correlation to vax rate.
We are reasonably sure my daughter got it on the flights or in the airport traveling back from vacation, since none of the family members we spent the week with have gotten covid yet, and she hasn’t been out of our house since. That would put it at exactly 3 days almost to the hour for her symptoms to manifest.
Czech government plans to propose to the Central Crisis Staff that people who test positive on an antigen test be permitted to work anyway. Obviously, this will include teachers.
This should be grounds for a labor strike (if withdrawing the promised raise wasn’t enough) but the teacher’s union here has no balls what so ever.
It seems pretty certain that omicron is less dangerous from a bad-outcome standpoint for people who are vaxxed. Is that true for the unvaxxed as well? Like, is an unvaxxed person less likely to die from omicron than from delta? That’s probably also true right?
Seems pretty clear that it is also less dangerous for unvaxxed. It’s just the sheer numbers of infections that are filling up the hospitals. I guess if the hospitals truly do buckle, we could see more poor outcomes as a percent of sick just because proper care won’t be available.
We really need to start looking at total hospitalized population for all causes, and the increases from say Nov 2021 and Jan 2020, to unravel how much of the “with Covid” population is actually in the “not for Covid but because of Covid” group.
This would basically be “excess hospitalizations,” but it would have some limitations. For one, you’d probably need some kind of seasonal adjustment. But more importantly, hospitals can choose not to admit people if there’s no capacity, reschedule voluntary inpatient procedures, etc., so you might understate the COVID burden. A consistent definition of for-COVID would give you an internally consistent metric to track changes in COVID burden over time and between areas, even if it’s consistent misclassifying particular cases. For example, if 10% of COVID hospitalizations show up with apparently unrelated strokes or something, you get a result that’s consistently 90% of the true number, but you still have an informative metric for identifying when things are getting worse and which areas are hardest hit.
It’s really not that important. Hospitals are cutting elective procedures (which include important things like cancer surgeries). Total capacity is stretched, Staffing is near broken. That’s true regardless of with or for covid distinction, which is a far more fuzzy metric than you’d think.
I feel like the point that needs to be driven home is:
Omicron is looking like what would have happened if we had no lock downs in March of 2020. Imagine these types of case counts nationwide but the hospitalization and death rates of Covid in March/April of 2020.
Calling peak from cases is hard right now as countries can just be hitting their system capacity for processing positive cases (and that capacity is slightly waning through the wave due to people in the system getting ill). Hopefully it is peaking as their health system is also under a lot of pressure.
Right, in my earlier post I did acknowledge that it’s not clear whether it’s a peak in testing capacity or an actual peak, but the raw numbers definitely look to have peaked.