I wonder if the bad taste in the mouth from taking this while having covid is similar to the phenomenon of people who lose their sense of taste with Covid.
I think it’s the mercury supplements he is taking.
1 Like
The bad taste is from the anti vitals. I am mid 40s and some health isssues. When I got tested they asked if I wanted them. Said yes please
Got sick Saturday. Don’t feel great today but it’s improving
With hope I got a few more days and it clears up
6 Likes
Don’t think so. The drug is secreted through your saliva glands, causing the weird taste a couple hours after each dose.
1 Like

This study is based on single digit sample sizes of many of their conditions, and it’s a study of in vitro response rather than clinical outcomes.
Also, this figure leaves me feeling pretty skeptical:

Their claims of statistical significance depend a whole lot on a bunch of samples registering zilch for a T-cell response here. It seems way more likely that the assay failed at several points than that a vaccinated person e.g. had a modest but measured T-cell response against the Wuhan strain, literally no response against delta, and then a Wuhan-equivalent response to omicron? Seems way more likely that the experiment went awry in the middle.
1 Like
Single digit Covid studies is to Tony LaRussa sabermetrics.
2 Likes
The two professors from Imperial College (that’s real professors, not the free-with-a box-of-cereal variety) understand statistical significance perfectly fine.
1 Like
the 5% seems strange to me. Anecdotally I don’t know of someone who hasn’t reported it. Like 5 for 5.
Yes, Wookie, did you realize that this study was authored by scientists from the Imperial College of London? You must not have, otherwise you would have realized that it is infallible.
1 Like
Just read it online somewhere. Sucks that everyone has to taste this.
So that’s a “no” on whether you read the actual paper critically and examined any of its claims. OK.
1 Like
The fact that you think academic professors automatically just know how statistics work is pretty damn funny and illustrates nicely how little academic experience you have.
1 Like
Previously infection-naïve HCW who became infected during the B.1.1.529 wave showed enhanced immunity against earlier variants, but reduced nAb potency and T cell responses against B.1.1.529 itself
I’m out of my depth here but that seems like a weird outcome. Do we think it’s legit? Does this ever happen with other bugs?
most dystopian covid thing happened to me this morning
was ordering some coffee and a bagel and i was talking to the lady and i wanted to dictate into my phone - from WFH for so long I instinctively will hit mute when I’m talking to someone else mid-meeting with the assumption the meeting can’t hear me because I’m on mute. apparently I got so used to doing this I “muted” the girl at the counter in my head and spoke into my phone like she wasn’t able to hear me.
god help us.
2 Likes
I can’t speak for where you live but they do here.
They aren’t jal. Academics are specialists in their field, not statistics. If you had any actual experience in academics, you would know this.
One of my companies had 30 some PhDs. I’m no stats expert but the we’re trying to discern 2-3% difference when the standard error was close to 10%. The also would keep running the same fermentation over and over to get the “best” result 3 times so they could report progress to the board. In reality all they were doing was showing the +2 standard deviation outliers.
I had to guilt them into tightening up all their measurements, running replicates, checking for hysteresis (eg things are all better or all worse in a particular week) and other stats 101 stuff.
3 Likes
Put in me in that category. I used to have to constantly remind myself of various stats stuff, and I’ve sworn to do no more research without getting paid… so now I don’t do much research despite being a prof. Just teach.
This is worded in a confusing manner. Here’s the data:
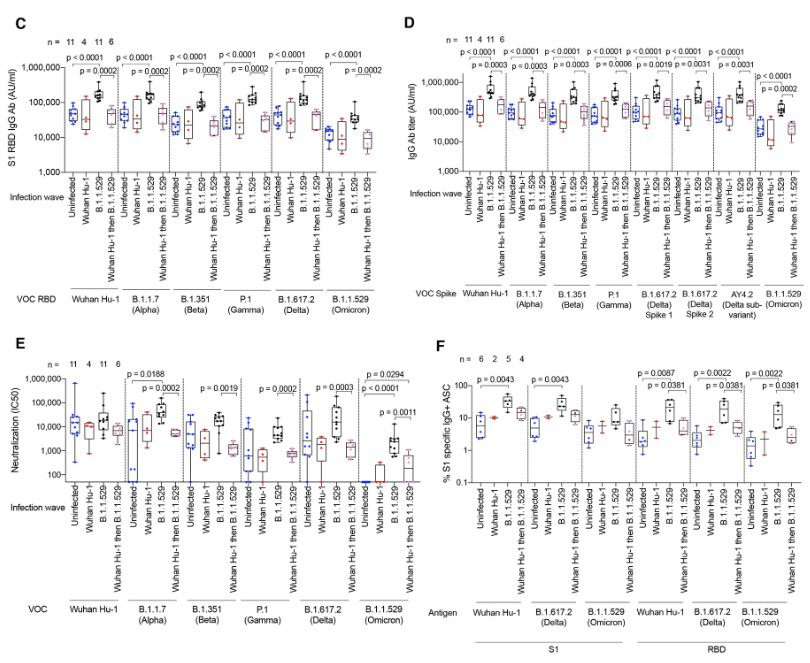
Sera from four classes of people (classes containing as few as 2 and as many as 11 individuals per class) are checked for response to viral RBD (C), spike protein (D), whole viral isolates (E), or T-cell response (F). These people are all health care workers, all triple vaxxed, and then have either been uninfected, or previously infected with Wuhan, omicron, or both. They check the responses of the sera from these people against Wuhan, alpha, beta, gamma, delta, and omicron variants of the 4 things above. It’s easiest to see if you look just at the black box plots, people who caught omicron only. Their sera have strong responses to the various conditions, usually the strongest of any of the 4 classes of people. Oddly, their response to omicron variants is less than their response against their response against other variants, but their response against omicron is still, at least usually, higher than that of uninfected patients. So, no, it’s not that a past omicron infection offers no appreciable boost to the immune response against omicron, it’s that in the purely academic case of measuring the boost against gamma (which basically doesn’t exist anymore) vs. the boost against omicron, it was observed here that the boost against gamma was larger.
This is probably because, these people all being vaccinated against Wuhan, their immune systems relied on anti-Wuhan antibodies rather than generating new ones. These were all very effective against all past strains, but less so against omicron.
It is somewhat weird that people who have caught Wuhan and omicron both aren’t showing much of an immune response relative to uninfected people except maybe sorta if you squint at the T-cell data, but the sample sizes here are just so small that it’s hard to be sure of anything.
2 Likes
You don’t need to be an expert in statistics to run p and t and chi tests. lol