Not great news
New data suggests these variants may have evolved to refavour infecting lung tissue, which could make them more dangerous.
So what can we expect in the coming weeks and months?
Although BA.2 continues to account for the bulk of UK infections, data from the Office for National Statistics up to 2 June suggests that Covid cases may be starting to rise again in England and Northern Ireland, driven by an increase in BA.4 and BA.5 infections. The trends were uncertain in Wales and Scotland.
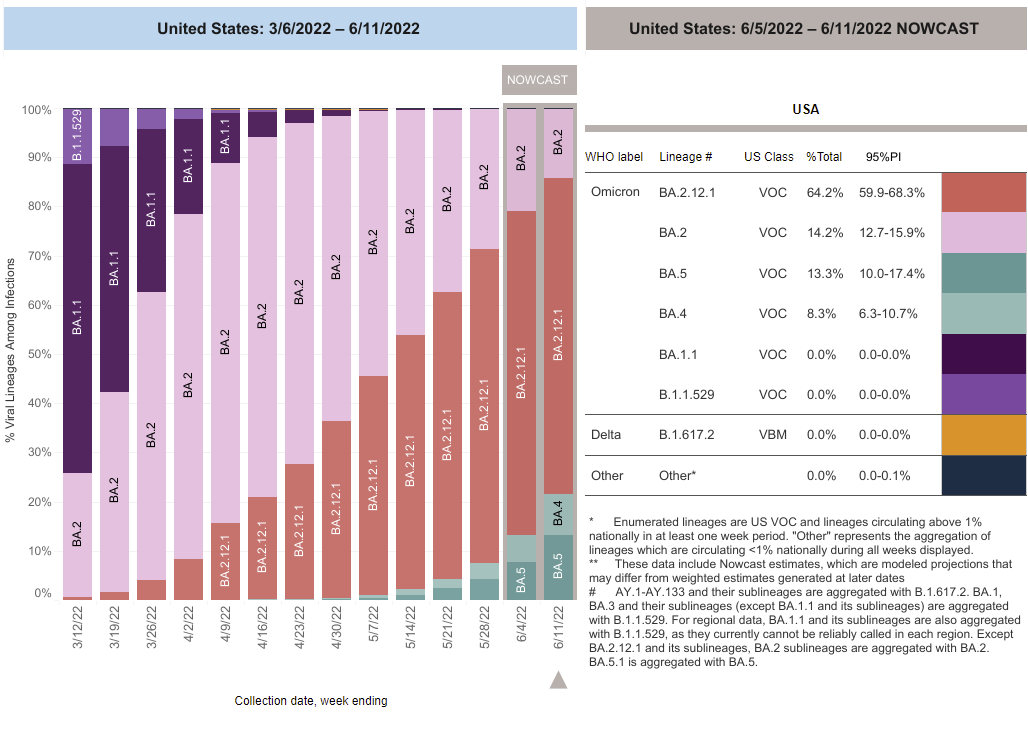
Also gaining ground in the UK are BA.5.1 (a child of BA.5), and the BA.2.12.1 subvariant (the USA’s dominant Covid strain), which the UK Health Security Agency is monitoring.
BA.4 and BA.5 were officially designated variants of concern (VOC) in the UK on 20 May, having first been detected in South Africa during January and February of this year.
According to the latest ONS data, about one in 70 people in England were estimated to have Covid in the week leading up to 2 June. In Northern Ireland it was about one in 65, in Wales about one in 75 and in Scotland about one in 40.
In South Africa, BA.4 and BA.5 have been responsible for a second wave of Omicron infections beginning at the start of May, which now appears to be flattening off. However, South Africa wasn’t hit by the highly transmissible BA.2 variant in the same way the UK was, and scientists had hoped that high levels of immunity from recent infection with BA.2 and booster vaccines might be enough to prevent these newer variants from gaining a significant foothold here.
However, with immunity from third vaccine doses waning in most population groups, and only the over-75s, and extremely vulnerable groups having been offered “spring booster” doses, this cannot be guaranteed. Neither is recent infection with the BA.1 or BA.2 Omicron variants necessarily protection against reinfection with BA.4 or BA.5.
According to research published in Science on Tuesday, natural infection with Omicron doesn’t produce a strong immune response, regardless of whether scientists look at antibodies or T-cells – meaning that people who have already recovered from an Omicron infection can quickly become reinfected. The findings, from Prof Danny Altmann at Imperial College London and colleagues, may help to explain why infection levels have remained high in countries such as the UK, despite so many already having been infected with it.
According to preliminary data from Kei Sato at the University of Tokyo and colleagues, BA.4, BA.5 and BA.2.12.1 may have evolved to refavour infection of lung cells, rather than upper respiratory tract tissue – making them more similar to earlier variants, such as Alpha or Delta. The propensity of earlier Omicron variants to prefer infecting non-lung tissue may be one reason why infections tend to be milder in most people.