Steven Millman Update:
January 23rd COVID Update: FINALLY some good news.
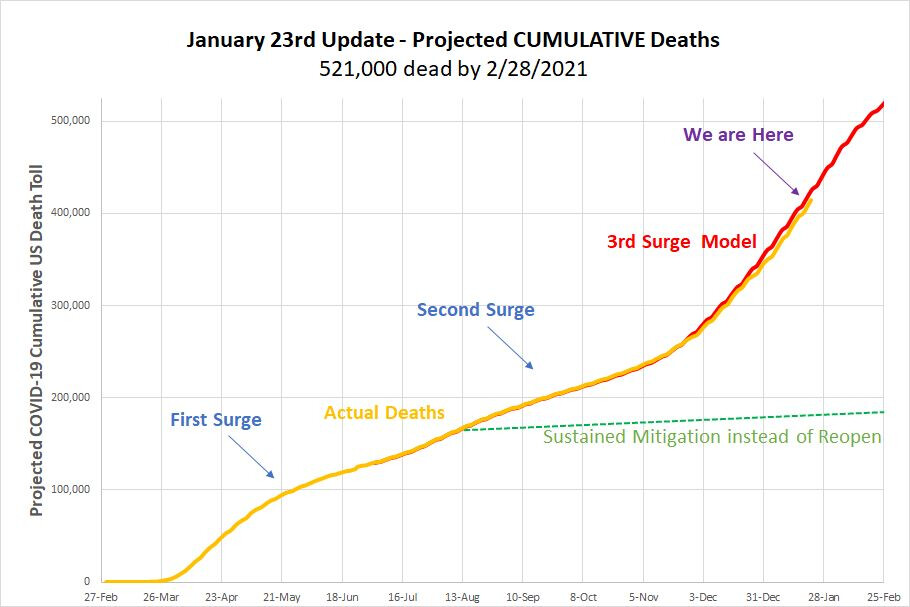
Short version: The increase in death rates will peak around Groundhog’s Day and then drop precipitously for several weeks. There are too many unknowns to look out farther.
tl;dr as ever. What’s that strange feeling I can’t quite place. Like some distant memory. Is it hope?
Federal government officials are now telling us that things are going to get worse before they get better and for a change they’re right. The average weekly death rate has been rising since early October when about 5,000 people were dying per week to the current state where just under 22,000 died in the just last seven days. The model projections suggest these numbers will continue to rise until the first week of February. The good news is that at that point there is very strong evidence that death rate will not only start to fall, but that they will fall rapidly. What we’re seeing right now at the national level is a substantial decline of both new cases and test positivity without a concurrent increase in testing. In combination these indicate a decline in community spread of the disease. That’s REALLY GOOD news. What’s not good news is that if model performance continues to be as accurate a it’s been thus far, January will be by far the deadliest month of the pandemic. The model estimate for January is 96,290 deaths from COVID in the US compared to 82,000 in December, 41,000 in November, and 23,500 in October. The model predicts that 72,000 will die in February, registering the first decline in death totals since mid-September.
We’re not out of it yet, of course. The model suggests that between now and the end of February, another 100,000 Americans will die from COVID. More Americans have died from COIVD so far than the entire population of Tampa, Florida. By the end of February, more Americans will have died than the population of Atlanta, Georgia.
I have only projected out to the end of February because there are far too many unknown variables about what will happen as well as a lack of clarity as to the key drivers of the decline in new cases we’re seeing now. There are a number of things happening that could continue to drive the number down. First, let’s consider the number of people who are currently at least somewhat resistant to the virus. There are about 25 million Americans who have had confirmed cases of COVID-19. Estimates of total community spread have ranged in the literature quite a bit, although most range between five and eight times the number of those confirmed by testing. If true, that means that between 125 and 200 million Americans have already been infected at this point. We know that reinfection is possible, that resistance from prior infection is of unclear duration, and that there is always the chance that a strain will mutate in a way that’s resistant to existing antibodies. That said, the total number of available hosts for COVID is probably only about half the population right now. This is nowhere near the level necessary for herd immunity, but it does greatly reduce the available source of people for the virus to infect – at least for a time. Add to those numbers the fact that about 16 million vaccines have been delivered, although only three million people have yet had two doses for maximum disease resistance. Vaccine distribution is slower than we’d prefer, but still progressing and focused principally on those at highest risk of mortality. Taken together, this suggests that there will be smaller and smaller numbers of available hosts, and that those who become infected will be at lower risk of mortality. Case fatality rate has held constant at about 1.4-1.5% for the last two months, and we would hope that number will start to fall in the near future as the size of the most vulnerable populations gets smaller . Finally, the change in administration messaging on the pandemic and what should be done about it (wear a mask, take the vaccine) could create a change in the acceptance of taking the simple steps necessary to reduce disease spread. The President has, for example, signed new executive orders requiring all persons in federal buildings to wear masks, and to require all persons traveling by planes, trains, etc. wear masks. These new rules, if followed, should have a substantial impact on disease mitigation. There are a variety of other disease mitigation strategies the President hopes to undertake, but it’s too early to know which of these will be funded and how effectively they would be implemented.
On the scary side, the new UK variant of the coronavirus appears to be much more transmissible than the original virus, between 30% and 70% moreso. This variant is expected to be the dominant variant in the US by March and that will drive infection rates up. Even more frightening, there is preliminary evidence coming out of the UK that new variant is also perhaps 30% more deadly as well. Mortality data for the new variant are too early to be reliable.
All in, its still too soon to know what will happen to disease spread and mortality in March and beyond. Remember, IT IS IN OUR CONTROL WHAT PATH THE VIRUS TAKES. If we ALL social distance, wear masks, and take the vaccine when it becomes available, this virus would be largely under control in about six weeks. This has always been true. We just need to do the things we obviously need to do, and then take the vaccine to ensure the virus can’t come roaring back.
But as it stands, 100,000 people will die in the next five weeks. There is, finally, hope – but that hope will be dashed if we don’t each do our own small part.
As always, not a medical professional, just a professional statistician that hopes there may be a light at the end of this tunnel.
Citations:
Johns Hopkins University CSSE / CCI; Updated: 01/23/2021, https://91-divoc.com/pages/covid-visualization/index.html
https://academic.oup.com/…/10.1093/cid/ciaa1780/6000389
https://www.economist.com/…/almost-one-in-five…
https://www.washingtonpost.com/…/1b55ff20-ee73-47cd…
https://www.bbc.com/news/health-55768627