I suspect that the US death curve won’t shoot way up like it is in the UK because we continued to burn through like 5k corpses a week the whole time, where they got their death toll down close to zero before things blew up again. We harvest our vulnerable daily, where most decent societies tried to protect them for as long as they could. Cool.
2 Likes
So I’m skeptical of the “treatment being better” idea. It’s possible sure, but the big things have been the same since late april or may.
3 Likes
Take a look at the slope of hospitalization rise.
https://twitter.com/covid19tracking/status/1323068320829112320?s=21
1 Like
100%, the deaths are coming. We can keep these people alive for a long time. We torture a lot of people on their way out.
5 Likes
This. My mother said if she gets covid don’t put her in the hospital because she’d rather die quicker.
I can’t get over how a whole years worth of progress against Covid was missed.
This seems weird coming from you of all people. Didn’t you point out that all sorts of things were being done early on that seem completely donkish now (e.g., early ventillation, not anticoagulating enough, etc.)?
Unless you’re saying that stuff was worked out by May and we haven’t come up with anything else. If that’s the case, I’ll take your word for it.
1 Like
More the latter. Since anticoagulation took hold in march and the recovery trial, nothing else has shown mortality benefits. There will be a learning curve in how to manage these patients, but I don’t buy that there’s been some massive shift in how we’ve treated this since June/July.
1 Like
IIRC, we have actual ER professionals in this forum who have attested to the fact that we’ve gotten better at treating COVID patients.
I’m one of them.
I’m tired. Coming off a long string of nights and trying to flip my schedule back to days. I don’t think I’m being very clear.
We’re better at treating now than we were in March and April, by a lot. That doesn’t even get into how NYC was utterly overrun and deaths come because of that.
However, since about April/May, there hasn’t been any big jumps. It takes a bit for those lessons to be truly learned elsewhere, but by June/July most everyone should be using those strategies at least some. The big jump in deaths is coming because we haven’t made those big changes. It’s just delayed because it takes a week or two minimum to die if you employ these methods usually if you don’t throw some massive blood clot in your lungs as your presenting symptom.
11 Likes
Well, shit.
1 Like
Well, if you want some optimism, nursing homes have changed how they do business so that should help more than anything else.
1 Like
That has more to do with demographics than covid care?
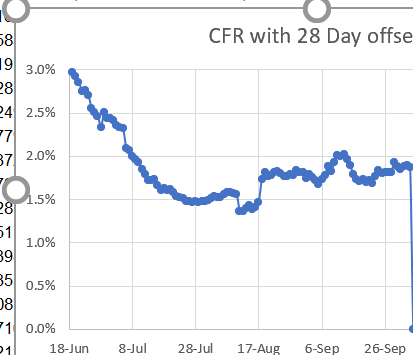
I’ll try to see how the offset cfr has been trending tomorrow.
IMO yeah. I’ve looked at zero data to support this, but nursing homes had little to no infection control before this. They were super vulnerable early on.
1 Like
I’m not remotely a medical professional, but the data points to a pretty consistent CFR since early July, which is consistent with @CaffeineNeeded’s post here.
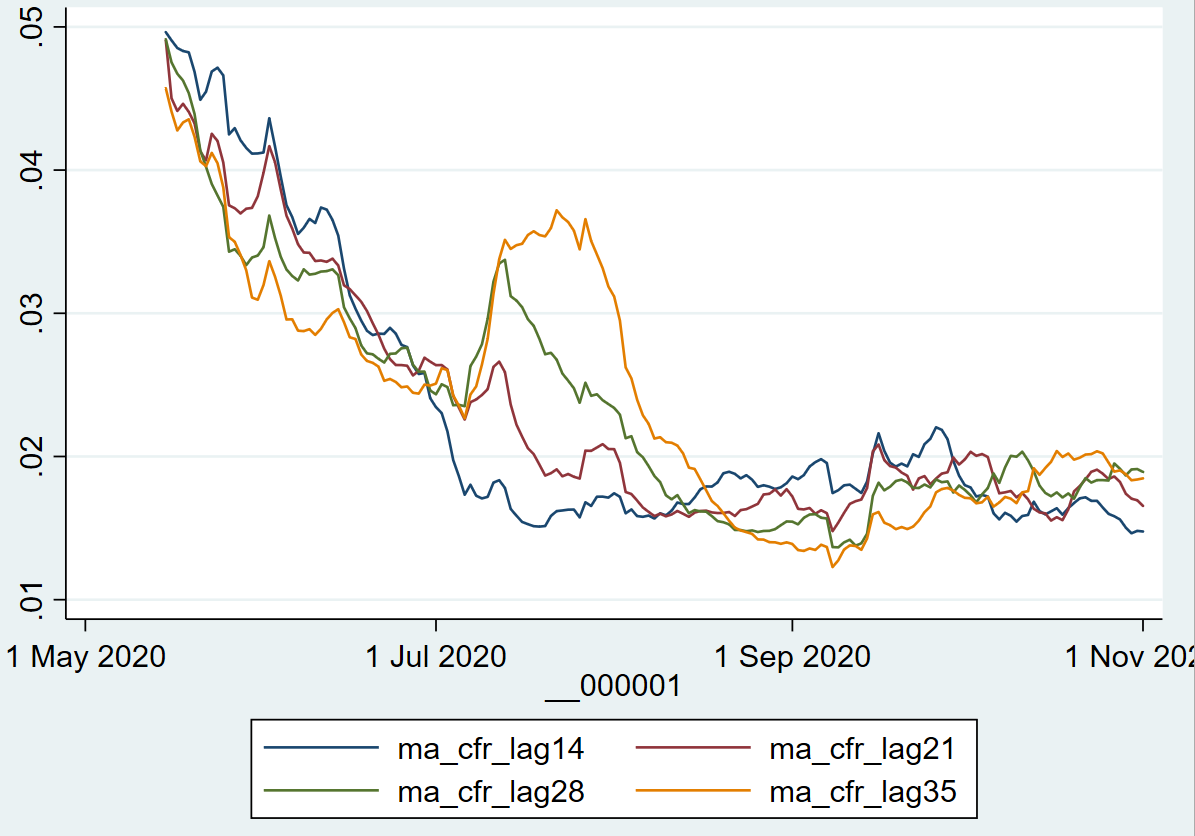
(Graph just shows estimated CFRs based on different lags between current deaths and lagged cases.)
The maroon line (7-day average daily deaths divided by 7-day average positive cases from 21 days prior) hit 2% or so in early July and it’s been around 1.5%-2.0% since then. And that includes the combination of better treatment AND positive cases comprising less-at-risk demographics. So it would be hard for me to believe that we’ve been making continual improvements in treatment since July.
11 Likes
What part of rounding the corner do you haters not understand?
Thanks for doing the work to show that.
4 Likes
This is potentially a huge deal. It obviously needs to be tested to confirm the results, but we’re talking free, instant tests on demand. Less burdensome than a temperature check, but 98% sensitive.
The paper is here:
One potential hurdle is that the false positive rate is very high (17%) for asymptomatic patients, which may limit its usefulness as a screening tool. One question is whether that value can be tuned down without completely cratering sensitivity. Or perhaps more training data can improve the numbers?
Pretty stable, if anything a slight upward trend the past 6 weeks. 1.9% So with current 100k cases we are looking at high 1,000 deaths/day unless anything changes. Can easily see another 100k through the end of the year.
1 Like
Yeah, for such a rapid and cheap test, a higher false positive rate is not that bad, and much preferable to a higher false negative rate, as long as people have a modicum of responsibility. A quick test that can get people to isolate and get a better test is valuable.
1 Like