Australia has its priorities right. Pubs and Restaurants can have 50 diners. Sitting only and properly spaced. Churches can only have 10 people because there is no economic reason to increase that number.
This is also basically where employer sponsored pensions came from.
https://twitter.com/BrianSimsPA/status/1265787518974377991
this is the PA house, republicans didn’t tell dems one of their members was positive for a week. yes, nothing matters.
2 Likes
come on guy
Why do you sound so certain about this? They might find better treatments before a year, but there is no guarantee that they will. We have to spend some time planning for the possibility that they don’t. That doesn’t mean open up everything now, but it does mean that maybe we have to plan a schedule for opening up things before there is a vaccine or herd immunity.
1 Like
Doctors and such, are treatments generally easier than vaccines?
Cmon man, take a breath. We all (I think) respect your position, but I postulate that not everyone that has introduced some additional level of risk into their lives is doing so for trivial reasons.
I speculate that the probability that this doesn’t happen is greater than the probability that COVID-19 originated in a Chinese lab.
Not a Dr but I would lay money that treatments will get better. Better enough to make a significant difference is the wildcard. Assuming no worse strain and no overwhelmed local hospital system, the later you get this thing the better.
Just guessing here, something like this within early 2021:
75% to improve 5%
50% to improve 10%
25% to improve 15%
Improvements is less deaths/hospitalizations.
1 Like
I’m hoping for better treatments because that would be the quickest way to help with public confidence. And I’m no doctor and have no expertise, but just the fact that it has a wide array of symptoms, some of which kill pretty quickly, leaves me skeptical. Would they be treating the virus itself or the pneumonia and other things it triggers? And it seems like early diagnosis and treatment would be keys to success.
Thoughts on risk:
I think understanding your location metrics are important.
Active Case density and local trend?
Is anyone in your social/work circle infected or quarantined? What about your local hospital(s).
How is behavior? Mask compliance?
If you associate with other people will they play by the rules? How sure are you that their risk profile is similar to yours? (And conversely did you increase your risk in the past 14 days like I did at Cheesecake Factory).
If it’s a work situation can you help improve with physical barriers, ventilation, low occupancy, etc?
1 Like
Yeah, I have a cousin who lives and works and pays taxes in Canada, she somehow got a double stimulus, and then also the Canadian stimulus. This administration is hugely incompetent. Don’t lie at any step, but it can’t hurt to apply.
This feels like a false dichotomy, where you want the choices to be open schools fully or keep them closed. You seem to be stridently against even talking about the possibility of a third option, as if coming up with one will shatter your world by invalidating everything you have done so far.
I’m not a doctor nor is this really my area of expertise, but it’s not really the realm of doctors, either. Administering drugs is a lot different from finding, designing, testing, and making them.
I would bet on a vaccine coming out well before a therapudic that outperforms remdesivir. Vaccines have a much clearer path to both safety and efficacy: get some sort of inactive form or part of the virus, show that it generates an immune response and not the disease, done. For a therapudic, you’re trying to come up with a small molecule ex nihilo that somehow inhibits a viral protein (or other biomolecule, but most likely protein) interaction but that doesn’t also inhibit something in the host. The easiest route here is to take a battery of drugs that already exist and that have proven acceptably safe on balance (obviously there’s a difference in safety between aspirin and chemotherapy drugs) and screen them for efficacy against the virus in cell cultures. This actually looks to be where the hydroxychloroquine hype came from: it was shown to be effective in cell culture against OG SARS. Obviously, that doesn’t always translate to in vivo efficacy, but it’s a good place to start if you’ve already demonstrated safety.
The chances of a novel compound being identified, and then shown to be both safe and effective? Small, and it would take years in the best case scenario. Don’t hold your breath.
I guess if you mean “treatment” in the sense of something that can address symptoms, like ventilators, we have some halfassed measures, like ventilators, right now, but I don’t think that’s what you mean.
1 Like
I concur on the magical thinking piece
We don’t have it here we are unique somehow
Kids can’t get it
Kids can’t spread it
These things always get weaker
Rural areas are safe
Six feet will keep me safe (better check what direction air is moving dipshit)
Everyone in my family/friend circle is safe so therefore it’s safe
Vaccine is gonna save us
Drug on tv is gonna save us
The reality is that we are opening up just when we started to get a handle on this thing in the hardest hit areas. It’s constant or increasing in many of the unaffected areas up to now. Putting sports teams together and opening schools is insanity but it’s going to happen.
2 Likes
https://dph.georgia.gov/covid-19-daily-status-report
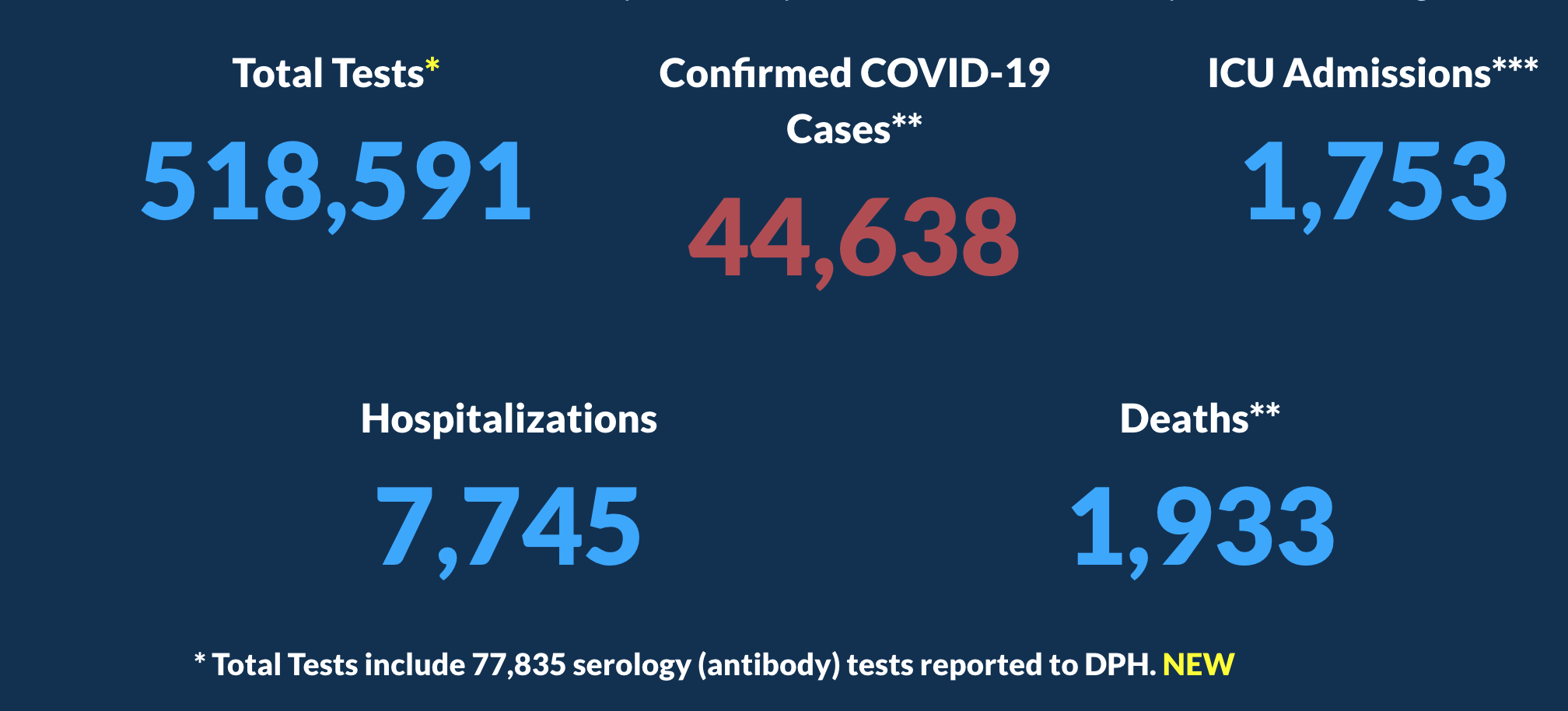
Georgia has started splitting out their serology tests now.
Which leads to this funny entry on covidtracking.com:

Except the problem is I still am not sure if we know which positive tests were from serology.
You’re right. I should have qualified about antibody treatments, which, in a sense, are very similar to vaccines, the goal of which is also to generate antibodies. My “novel compound” was meant to refer more specifically to “novel small molecule compound,” while antibodies are protein complexes. Antibodies have a very clear path to production like vaccines, except instead of producing the thing that stimulates antibodies, you just produce the antibodies. It tends to be much more costly to produce antibodies at scale, even if it’s pretty easy to get a handful of doses from a recovered patient. I don’t think we get to 7 billion doses this way, but it could save some lives along the way. This article is paywalled, but if you happen to have access, it’s another bit of interesting work on antibody therapy development:
2 Likes
From what I’m reading this new COVID mutates at a very slow rate for an RNA virus, and in particular this “spike” protein that helps it bind to lung cells is particularly conserved, which is all good news for the prospect of a vaccine.
3 Likes
It sounds like we’ll know more in two months when trials are completed. He seems like a legit guy. Long-term, I think a proper vaccine is preferable to treatment, but this seems promising.
1 Like
But we AREN’T doing that. We are just opening fucking everything. That isn’t a plan, and we are going to be mighty fucked because of it, probably to a worse extent than we already are.