For some reason a large ivermectin study was done.
In shocking news, it doesn’t work.
https://twitter.com/peterhotez/status/1505138376218972167?s=21
For some reason a large ivermectin study was done.
In shocking news, it doesn’t work.
https://twitter.com/peterhotez/status/1505138376218972167?s=21
That’s what they want you to think so that the Globalists can keep the ivermectin for themselves (and their horses)!
Shit, gotta go get tested for COVID. I feel some symptoms.
I mean I hope it’s just allergies most but the symptoms are the same that I felt after getting the second covid shot. Except I’m coughing a bit and don’t have a fever this time.
Have you heard about a single horse dying of Covid. Make you think, huh?
Everyone knows horses aren’t real. WAKE UP SHEEPLE!
Negative after eating indoors a bunch in Bulgaria. Got home last night.
EDIT: In comes the fever. 100F
Antigen test came back negative. However, I might have taken the test too early in the course of the infection (only been day 2 of symptoms).
PCR test is expected back tomorrow.
No idea what the symptoms are the result of I guess but given the removal of basically all COVID restrictions in the CR starting last Monday and the fact that I work in a school, it’s probably COVID.
There have been a few studies, and I think they generally show not amazing results for young kids. A summary of the data from one preprint:
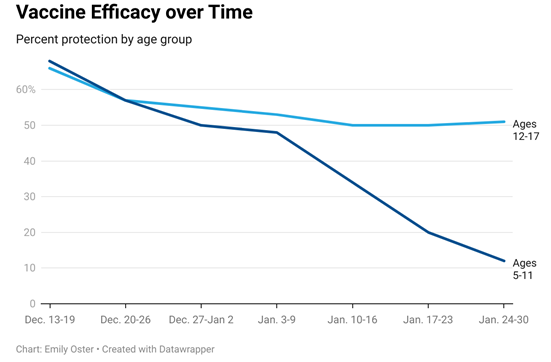
(This is an easier-to-read version of the data from Figure 1 of the preprint)
From a recent CDC release:
Children and adolescents aged 5–15 years were tested for SARS-CoV-2 weekly, irrespective of symptoms, during July 2021–February 2022. Approximately one half of Omicron infections in unvaccinated children and adolescents were asymptomatic. Two doses of Pfizer-BioNTech COVID-19 vaccine reduced the risk of Omicron infection by 31% among children aged 5–11 years and by 59% among persons aged 12–15 years.
So that doesn’t seem great, but there’s a really big confidence interval around that estimate, so I’m not sure how seriously to take it.
I think the most likely story is one that Katelyn Jetelina offered a couple of weeks ago:
Vaccine dosage matters . What was surprising is how quickly VE waned among 5-11 year olds compared to 12+ year olds. This suggests that dosage could matter a lot . In fact, it confirms results from an August 2021 primate study that showed that dosage significantly predicted upper and lower airway viral replication in monkeys: the higher the dosage, the lower replication. (Interestingly, the authors of this primate study created the Moderna vaccine, which may explain why Moderna went with the higher dosage approach, compared to Pfizer, which went with a lower dosage approach in their vaccines.)
This is consistent with Pfizer’s <5 results being so weak - they (compared to Moderna) intentionally targeted a lower dosage for kids because they were more focused on potential side effects than efficacy. Moderna has been willing to risk higher side effects in exchange for higher efficacy.
I’ve got an 11 year old and my current strategy is to get a regular shot when he turns 12 in a few months, rather than getting him boosted with the weaker 5-11 shot.
An alternative explanation is that the paper is a cohort analysis, so there’s all sorts of confounding variables. A simple thing like ‘kids who got vaccines were more likely to get tested or have some sort of medical condition’ could submarine that entire analysis if not properly accounted for. You can try to account for this, but it’s not something that is going to be apparent in population level data that they used.
Last week I tested positive on an antigen-test a couple of hours after I woke up with symptoms. Second antigen-test and PCR test confirmed.
I remember my sister being told to wait a few days after getting symptoms because the tests would be more reliable then. Since waiting a few days after symptoms for me would involve going to work in a school with COVID, I opted against that.
Given that the symptoms have got worse since the tests, I’ll probably miss Monday even if the PCR test comes back negative. Even if I don’t have COVID, I still won’t want to go to school.
It’s hard to disentangle why a test returns a false negative, whether it was a faulty test or if the person truly had sub-detection-limit amounts of the substance in question (viral antigens, viral RNA, etc.), but in general, most people who have recently developed symptoms should have detectable amounts of the stuff. Viral load tends to peak before symptoms, not after.
For +12 months in the UK we have known a home test will show when you’re contagious and a PCR will show positivity earlier and after you’re contagious when a home test won’t pick it up - maybe a Biden test is less reliable but you’re not testing positive on a home test 24hrs after meeting that contagious person because your not infectious at that point
This is wrong early in the disease. It’s not perfect outside of the beginning either. Stop giving bad medical advice.
Testing positive for COVID-19 means you have pieces of the virus in your body. However, a positive test does not always tell you whether or not you could spread the virus to other people. The test that uses a method called reverse transcription polymerase chain reaction (RT-PCR) to look for genetic material of the virus can return a positive result even after you no longer have an active infection but still have inactive (dead) pieces of virus in your body.
Another type of test for a current infection looks for proteins (antigens) from the novel coronavirus. If you receive a positive COVID-19 result from an antigen test and are experiencing symptoms, you are likely contagious.
That does not support your assertion. Your cite random paragraph rules in, it doesn’t rule out. Again, stop giving bad medical advice.
BTW the correct answer here is that if you’re rapid negative at the end of the disease, you’re likely not contagious, but it hasn’t been firmly established what the chances of you being contagious are afaik.
The issue is that early on you can change from ‘not contagious’ to ‘contagious’ very quickly as viral replication goes through exponential growth. Using rapid tests to determine whether or not you’re infectious early on is not a good idea.
Please do not be confused with my advice - this is not a medial forum, I am not presenting a study, so this is not medical advice (much like your advice)
It is well established you will test postive earlier and well after a covid infection via PCR than you will with anitgen test - even people not working in the medical field know this
This why countless governments around the world let you end a period of isolation off the back of a negative antigen test and don’t require a PCR test to re-enter the population - otherwise, what’s the point of a Biden Test.
Exactly churchill, end a period of isolation. That’s the important part here. Advising someone that they don’t have to isolate with new active symptoms for 24-48 hours based on a rapid is flat wrong and bad advice.
Lols, I wasn’t advising that Ikes - now I see your confusion - I was stating a ‘negative rapid test’ taken within 24hrs of a malady without fever doesn’t necessarily mean you’re negative or that it’s a ‘false positive’ - just that a rapid test would never pick it up this quick.
Biden should have sent some basic instructions with those tests - might be why they take 48+ hours to arrive, I guess.