and? It is.
Ah glad you’re the arbiter.
Video has Dr Charles Shepherd who can explain to you how he suffers from ME/CFS himself.
Probably worth listening to what this experienced doctor has to say about how he contracted it while working as a hospital doctor.
1 Like
Was it Social Media Brain?
4 Likes
nope, it’s not.
NHS so questionable source
Sharpe didn’t ‘catch’ CFS/ME.
He’s also a major author on a paper claiming a psych component to CFS/ME. The treatment section of his link literally suggests cognitive behavioral therapy. That’s a weird thing to suggest for a disease that’s purely ‘medical’. Jal is clearly trolling.
Not sure what the point is carrying on here.
Well it’s not black and white is it … like a lot of medicine. Experts disagree. And yes I’m just some plebian on the matter but I am of the view that it’s insulting to dismiss it as psychological (it cheapens the real physical symptoms in my experience). The fact that the initial publisher on this suggests this doesn’t mean he’s right. Also the video is Shepherd not Sharpe so unsure what that point was. Anyway, I’ll leave it because debate in this thread invariably ends badly. I just felt the foolish urge to weigh in given I’ve seen how awful it is up close and personal.
Saying it’s psychological isn’t dismissing it. That’s your bias showing up and something you should think about. Debilitating psychological symptoms are still debilitating and still are very real.
My problem isn’t that you disagree. My problem is that obvious bad faith bullshit from Jal who took this opportunity to fight in obvious bad faith. There’s no other explanation for taking a strident position that something isn’t psych related and then posting a source that suggests psych treatment and suggesting that he caught it as a doctor working in a hospital (which I just happen to do). I’m tired of the constant bullshit, and I find this topic actually quite interesting.
1 Like
I am not in any way qualified to weigh in on MECFS but I don’t think it’s helpful to frame it as a dichotomy in such loaded terms.
Some afflictions are more psychological than physiological in nature. Stigmatizing people who suffer from the former rather than latter as nuts is why mental health is still a taboo subject and some reluctant to get help. Again, I am not taken a position here if MECFS is one or the other. Just speaking in general here.
6 Likes
I hesitated for a moment before liking this post because I didn’t want it to seem to make light of iron81’s illness but come on… that’s a funny post.
2 Likes
I don’t know who this Sharpe is you refer to.
Please stop insulting me by saying I’m trolling when I post an NHS video by a medical doctor with many years of experience in this area who believes he contracted CFS/ME after treating a patient.
Anyway, I’ll leave it at that.
That’s well said. As someone who repeated my Senior year (year 12) due to depression I empathise with psychological illness and the manifestation they have in physical terms. And maybe I am biased but my cousin has had these sort of psychological issues diagnosed and it always seems like such a loaded diagnosis. The treatment accompanying these has always failed dismally in her experience. Many things may play into this (her being a small, petite woman with a foreign accent in Australia and being treated by white boomer doctors for the most part). I just don’t see the illness in such black and white terms as I don’t see many illnesses (I’m sure more than most people) in those terms. I can’t really weigh in on Jal’s post I just appreciated that the NHS has a page on it discussing it in detail. That legitimises it for a lot of laypeople. Yes it prescribes psychological treatment (among many other things which I consider more relevant/effective) which I disagree with but again black/white etc etc.
2 Likes
The more you think about it the less sense this distinction makes.
If your heart isn’t working properly, that’s physiological. But if your brain isn’t working properly, that’s not physiological?
3 Likes
Totally agree, but the ME/CFS community flipped the shit at an RCT showing improvement (even if it wasn’t the best trial) precisely because of their rejection of the idea it could be psychological or that going after symptoms of a disease was appropriately. It’s a weird dynamic.
I agree with you that it’s hard to delineate them. Maybe it makes sense to look at the root cause. Let’s take PTSD for example. It’s “real”, it might have physiological manifestations but the best way to treat it is as far as I can tell by psychotherapy or related treatments.
I’m not knowledgeable enough to have an opinion on CFS/ME, but I know that just because a physician says, “I have it,” doesn’t make it so.
So a few things.
-
This group isn’t some thing all doctors vote on. This is very much ‘a group of experts’ scenario and not an actual consensus. I don’t think that document reflects, at all, what a typical doctor thinks about CFS/ME. Obviously that’s not rigorous, but it’s not exactly hard to find stories of people with CFS/ME who talk about how their doctors don’t believe them.
-
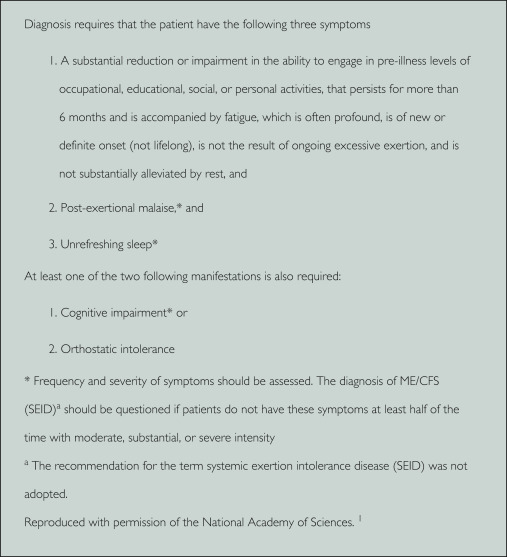
Look at the criteria closely. Let’s post them here so people can see them:
And then lets go to the DSM-V definition of major depressive disorder:
- Depressed mood most of the day, nearly every day.
- Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day.
- Significant weight loss when not dieting or weight gain, or decrease or increase in appetite nearly every day.
- A slowing down of thought and a reduction of physical movement (observable by others, not merely subjective feelings of restlessness or being slowed down).
- Fatigue or loss of energy nearly every day.
- Feelings of worthlessness or excessive or inappropriate guilt nearly every day.
- Diminished ability to think or concentrate, or indecisiveness, nearly every day.
- Recurrent thoughts of death, recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide.
There is a ton of overlap here. I don’t see how you can clearly separate the two. Even if we truly knew what CFS/ME actually was, it would be extremely difficult to differentiate MDD and other psychological disorders from CFS/ME. There’s also a whole set of people who claim this when it was the thing to have in the 00s/early 10s. Clearly delineating this is extremely difficult.
There’s been a ton of work to find some biological (used here to mean not psychiatric even though it’s all biological) and it has come up short. I’m not aware of any RCTs that have shown benefit for any of these treatments. If CFS/ME was some pure nervous system disorder, we should have drugs to make it worse or better.
The biggest thing I’ve seen is that the CFS/ME community find it appalling that they may have a psychiatric disorder, as their own biases force them to say that’s not possible because it would mean they have some sort of intrinsic failure that ‘biology’ does not. That’s bullshit. A real look into the cause wouldn’t start off with ruling out a major cause of disease.
1 Like
Suddenly a lot of the Covid opinions itt make sense to me.
2 Likes
CDC catches on to ‘longer gap between doses equals better effectiveness’ - 13 months later than other countries.
U.S. health officials said they are considering lengthening the recommended interval between the first two doses of the most widely used Covid-19 vaccines to eight weeks to lower the risk of heart inflammation and improve their effectiveness, Reuters reports.
Dr. Sara Oliver, an official at the U.S. Centers for Disease Control and Prevention (CDC), said the agency was considering making the recommendation for Moderna and Pfizer /BioNTech jabs during a meeting of the Advisory Committee on Immunization Practices, a panel of outside advisers to the CDC.
In the U.S., the recommended interval between the two Pfizer jabs is three weeks while it is four weeks for Moderna’s vaccine.