Also, NN Taleb. (I can’t articulate exactly what it is that he knows more about, but I’m certain that there are aspects of capital markets he knows more about.)
NN is kind of a douche, but that’s a little unexpected. It’s a bit surprising that you would feel completely comfortable ignoring his thoughts on those aspects of capital markets that you care about and that he knows more than you about. I’d have been sure you would be interested in what he said, even if you ultimately disagreed with it.
Not to derail this thread any more, but the problem is that I’m not actually sure what those areas are. I’ve read Fooled by Randomness and (I think) Black Swan, but I didn’t learn anything from either of them, other than he’s a pompous ass who simultaneously believes that:
- humans are incapable of properly evaluating the consequences of fat-tailed distributions
- we cannot judge individuals’ skills based on ex post outcomes
- he is able to systematically profit from his expert beliefs about fat-tailed distributions, and we know this because of his ex post results
I’m confident that he’s much smarter about pure math than I am and also that he knows much more about the logistics of managing a large portfolio of stocks and options. So I’m sure that I could learn things from him. It just hasn’t been worth dealing with all of the bloviating nonsense IMO.
To get this thread back on track, I’ll just note that all of my kids have now gotten both vaccine shots and my wife has joined me in the booster club. So we’re ready to start licking doorknobs or whatever.
1 Like
Congratulations. Also, fuck you and your old enough kids! I want to lick doorknobs too!
Science Journalism Fail of the Day goes to:
No, it fucking doesn’t. That’s not at all what that study found.
Wait wat? Sounds dirty.
1 Like
Pfizer CEO was interviewed today and indicated that they expect the final submitted data for Paxlovid to show the same as the interim results, an 89 percent reduction in the risk of hospitalization or death. It’s still a game changer, and they are shipping the pills out now and should be asking for authorization in the next few days. If doctor’s start prescribing this in a widespread manner this winter we should start to see hospitalization and death rates falling dramatically. Honestly, I think this is more of a game changer then even the vaccines were.
1 Like
I know NFTs are massively popular, but I was not expecting Pfizer to start dropping Pax
2 Likes
Would be cool given current circumstances if this doesnt go on the calendar for like a March 2022 approval.
1 Like
Forgive me if this is weird, but I don’t know this guy. Is he a doctor?
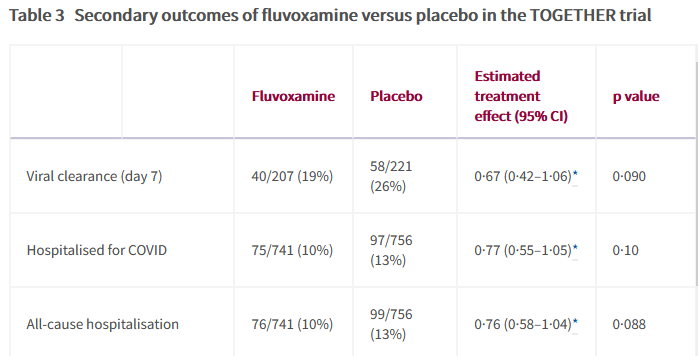
The RCT on fluvoxamine seemed great when I first saw the headlines, but on further review it’s not particularly a strong RCT. There actually is no difference in hospitalizations (p-value was 0.088) despite what this person says. There’s a difference in a composite measure that includes ER stays which shows a decrease, which is difference and tough to tell what it means exactly. There’s no mortality benefit.
It’s fine if you want to give it imo, but there’s not enough evidence to recommend it yet imo.
The newsletter is from Matt Yglesias, who is emphatically not a doctor. I’d be surprised if you don’t recognize the name, but in case you don’t he’s a generalist blogger who (imo) is smart across a variety of topics, smart enough to read and interpret relevant studies, but not someone with actual subject matter expertise in this area.
(I refer to him as Matty G, although I’m not sure why I started doing that. Was it a @anon10396289 thing?)
In terms of the actual study, I think (in general) treating a p-value as binary isn’t great. In particular, I really don’t agree with this interpretation:
There’s clearly a meaningful difference in hospitalizations between the two groups, and the question is whether that difference is a reliable one, rather than an artifact of noisy data. It’s true that many people automatically jump to a 5% p-value threshold, but there is no magic p-value threshold, and if you showed me these numbers and said that you couldn’t infer anything about Fluvoxamine and hospitalization rates because the p-values were <.1 rather than <.05, I think that would be a bad interpretation.
But if you view this as evidence in favor of Fluvoxamine, but not strong enough to recommend it yet, then I don’t disagree with you.
Be nice if Iggy talked to like a single health professional before chiding the FDA for not recommending this drug based on one study.
1 Like
Sure it’s evidence, but just remember there’s almost always a bias to benefit the treatment arm in this kind of study. Add in the mechanism of this is basically unknown, and it’s really not great evidence. This clearly falls into the ‘needs further study’ bin.
Answer is obviously same for soccer.
Delta passed to Omicron at midfield. A defender’s hand lightly grazed Omicron’s shoulder area. Omicron fell to the ground writhing in agony. Omicron is now receiving the magic spray on the sideline and ready to go back in.
3 Likes
With the inherent bias towards the treatment arms in medical literature, not really.
Just wanted to say that the discussion in this thread has really been good this past week, thanks to all for the updates.
2 Likes
Seems odd for the FDA to make recommendations based on any one study. Iggy seems to think it’s a quality study but I wonder if he’s qualified to make that call.
Surely he could call up Emily Oster and get her take.
My snippet may not have captured the spirit of the full post (here), but it’s more reasonable than you suggest.
Overall argument: Our public health agencies should be following the science (and are not)
Evidence:
- We continue to stick with the schedule of three weeks between vaccine doses, despite evidence that a longer gap is likely better.
- The FDA is delaying approval on COVID tests that are currently approved for use in other countries.
- The federal government’s official treatment guidelines have not been updated since April. So they continue to say this about Fluvoxamine, seemingly unaware of the RCT:
He’s not saying that the FDA should make a change in recommendation based on a single study with not-bulletproof results. But he is saying that the FDA should be incorporating studies like this into their decision-making, and they should (in appearance if not substance) look like they’re interested in making real-time decisions based on evolving data, rather than being the super slow to respond agency that Michael Lewis’s book did a good job describing.

I realize that this string of posts makes me seem like a crazed Fluvoxamine supporter. In reality, I had never heard of it before this morning. I just think that Matty G’s overall post was good and convincing, and I wanted to get some anecdotal thoughts from @CaffeineNeeded on whether or not he’s thought about using prescribing the drug.
2 Likes
lol matt yglesias, the guy who defends sweatshops and the Trail of Tears, who tut tuts the idea that some Americans could be suffering because averages are good. All around he’s a fucking idiot who shouldn’t be posted in this forum. He exists to give centrists cover for their hellacious policy.