Yeah, I think Tractor Supply has been posting warnings for a while now.
2 Likes
Its got a picture of a horse on the package! 
4 Likes
You can’t fool smart people who have DONE THEIR OWN RESEARCH with that second-rate imitation product that’s on sale. They’re going for the primo, top-shelf stuff.
3 Likes
I think it’s time to be done with “public comments.”
https://twitter.com/billycorben/status/1428831471960199174?s=21
Wait, WAT? I totally missed that. How exactly did they force docs to prescribe/administer ivermectin?
Well, humans are animals. Chessmate?
Before I go down a rabbit hole, maybe someone can ELI5 this for me.
Apparently, if you had SARS before, those antibodies are great against all known covid variants (only if in conjunction w/ vaccine?). What is so difficult about developing a vaccine that causes the production of those antibodies as well? I’m assuming there is a rub somewhere.
How is is that having SARS is more protective against COVID than having prior COVID? Is that even a true statement?
Gonna need to see the receipts on this one. Who didn’t think we’d need boosters? Maybe a debate about timing?
1 Like
By chance, I read a preprint of a paper yesterday that was very weird. It was an observational study in which COVID patients were dosed with azithromycin plus one of three drugs - nitazoxanide, ivermectin or hydroxychloroquine. All three regimens showed astonishing benefit, to the point where the authors flagged ethical concerns with proceeding with RCTs of the drugs. I skimmed through it, basically just filed it under “that makes no sense at all” and went on with my day. Lo and behold, today two blog posts dropped flagging what looks like obvious fraud in the underlying dataset:
https://gidmk.medium.com/is-ivermectin-for-covid-19-based-on-fraudulent-research-part-2-a4475523b4e4
They’re interesting reads to look at the kind of detective work which can demonstrate fraud - and they come at it from different angles, so both are worth reading.
The second piece is written by an Australian Ph. D. student in epidemiology calling himself Health Nerd, who I recommend following on twitter. This is part two of a series on fraud in the ivermectin literature. He says part three is coming soon ![]()
4 Likes
I only read the first one. Piping hot take incoming.
That first case doesn’t sound that bad. If there is some licensed doc that wants to administer it and it is something the patient wants to do, then I don’t think it’s that bad to allow those willing participants to engage in this idiocy. Assuming there is no liability for the hospital (which seems unlikely given they fought it), I don’t really have that much of a problem with it. But I can imagine that assumption may not be perfectly valid.
I’m also assuming that the fact that some licensed doc is willing to administer it means that it is not sufficiently egregious malpractice that they would lose their license for doing it.
I also understand why the hospital would fight it and there are very reasonable arguments why they should not be forced to allow this in their facility. However, the fact that they lost this one doesn’t rustle my jimmies that much.
Flame on.
Over nighting in northern Idaho on our way to the badlands. The only fucking people wearing a mask in this state are my daughter, my wife and me.
3 Likes
So like 30%? Better than Ohio.
9 Likes
Isn’t there like a fuckton of wildfire smoke out there?
Not a flame, but if your well meaning local doctor is basing their use of the drug based on fraud, then it does matter. I read the second paper and a couple of it’s linked articles and basically feel sick. The Egypt paper has already been retracted. The Brazil paper stinks like Jerry’s car. This goes way beyond bad science, poor controls, etc. outright make believe.
Dollars to donuts someone has speculated on ivermectin and is making a killing.
Really seems like some second and third world systems are buying in because they can tell patients that are doing “something”. Understandable but wholly indefensible.
1 Like
I think this is on the doc, though. I’m sure on occasion certain docs have certain views that are not mainstream but they act on them based on their knowledge and experience. And I assume the rare times they do this they have put significant effort into their decision-making processes.
And I’m good with that if they are very up front with the patient that their advice is unconventional or opposite of the standard advice or whatever the case may be. Maybe even go the extra mile and make sure they talk to someone with the more standard view.
Now in this case, unless this “well-meaning local doctor” is living under a rock, he should know for sure that “Ivermectin cures COVID” is not exactly mainstream. Hence, he should be very skeptical of the opposing view and with a bit of effort (which he damn well better expend if he is going to make such a recommendation) he should be able to conclude that those studies are shit.
Hospitals are also very much allowed to certify who does and doesn’t operate within their walls, this is especially true for ICU patients who are typically walled off from other doctors who can otherwise practice in the hospital. It’s a bad take. If it was some asshole in their office sure, but someone who isn’t credentialed and isn’t qualified for ICU? Fuck that.
1 Like
I think the bulk of places doing this are in places where people aren’t reading the literature themselves. Just lay articles written by folks that don’t know how to review the papers critically.
These things get accumulated into larger studies but it seems the bad ones have big samples sizes that make them outweigh the property done studies to the point of changing a negative result to a positive one.
Kind of like the mortgage bond fiasco. A few piles of stinking shit folded together become gold standard research.
While we’re doing a series on ivermectin fraud, there’s also this study from India investigating ivermectin for COVID prophylaxis. Ivermectin was given to around 63% of n = 3,532 staff at the hospital, basically whoever wanted it. The study purports to show a highly significant risk reduction in acquiring COVID-19.
There’s a Twitter thread here outlining a number of suspicious-looking issues with the data, but I’ll show one of the more amusing ones. 473 study participants were coded as having the occupation “student”. Here is their age distribution:
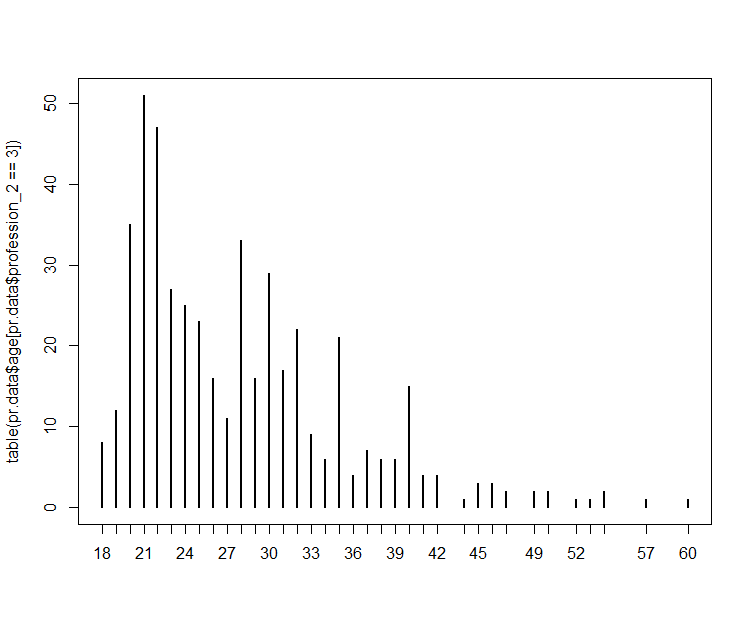
Note the suspicious spikes at exactly 35 and 40 and the median age of 28. Like the guy says on Twitter, wonderful to see such support for lifelong learning in India.
2 Likes
hey, i’m driving through idaho tomorrow! looking forward to being second household to mask there.
1 Like