No, I don’t want it to be my job to caveat all of your posts. I want you to be able to differentiate between “studies show” and “scientists are investigating.”
This (non peer-reviewed) study out of Rockefeller University is the only one I could find dealing with this issue.
I’m not an expert so can’t confidently interpret their language, but it seems to be saying that the effects of the new strains (UK, SA, Brazil) on general vaccine efficacy is fairly modest due to these vaccines’ polyclonal effects. I think Hancock might be confused between the new variant’s effect on the vaccine in general and its effect on certain antibodies that the vaccine provokes. Study abstract says:
Here we report on the antibody and memory B cell responses in a cohort of 20 volunteers who received either the Moderna (mRNA-1273) or Pfizer-BioNTech (BNT162b2) vaccines. Consistent with prior reports, 8 weeks after the second vaccine injection volunteers showed high levels of IgM, and IgG anti-SARS-CoV-2 spike protein (S), receptor binding domain (RBD) binding titers3,5. Moreover, the plasma neutralizing activity, and the relative numbers of RBD-specific memory B cells were equivalent to individuals who recovered from natural infection6,7. However, activity against SARS-CoV-2 variants encoding E484K or N501Y or the K417N:E484K:N501Y combination was reduced by a small but significant margin. Consistent with these findings, vaccine-elicited monoclonal antibodies (mAbs) potently neutralize SARS-CoV-2, targeting a number of different RBD epitopes epitopes in common with mAbs isolated from infected donors. Structural analyses of mAbs complexed with S trimer suggest that vaccine- and virus-encoded S adopts similar conformations to induce equivalent anti-RBD antibodies. However, neutralization by 14 of the 17 most potent mAbs tested was reduced or abolished by either K417N, or E484K, or N501Y mutations. Notably, the same mutations were selected when recombinant vesicular stomatitis virus (rVSV)/SARS-CoV-2 S was cultured in the presence of the vaccine elicited mAbs. Taken together the results suggest that the monoclonal antibodies in clinical use should be tested against newly arising variants, and that mRNA vaccines may need to be updated periodically to avoid potential loss of clinical efficacy.
Their conclusion seems to be that while current mutations don’t escape the current vaccine, their evolutionary trajectory seems to indicate that they eventually will and that vaccines may have to be tweaked in the future:
A number of circulating SARS-CoV-2 variants that have been associated with rapidly increasing case numbers and have particular prevalence in the UK (B1.1.7/501Y.V1), South Africa (501Y.V2) and Brazil (B1.1.28/501.V3)12,15,17,28,39. Our experiments indicate that these variants, and potentially others that carry K417N/T, E484K and N501Y mutations, can reduce the neutralization potency of vaccinee plasma. The comparatively modest effects of the mutations on viral sensitivity to plasma reflects the polyclonal nature of the neutralizing antibodies in vaccinee plasma. Nevertheless, emergence of these particular variants is consistent with the dominance of the class 1 and 2 antibody response in infected or vaccinated individuals and raises the possibility that they emerged in response to immune selection in individuals with non-sterilizing immunity. What the long-term effect of accumulation of mutations on the SARS-CoV-2 pandemic will be is not known, but the common cold coronavirus HCoV-229E evolves antigenic variants that are comparatively resistant to the older sera but remain sensitive to contemporaneous sera40. Thus, it is possible that these mutations and others that emerge in individuals with suboptimal or waning immunity will erode the effectiveness of natural and vaccine elicited immunity. The data suggests that SARS-CoV-2 vaccines may need to be updated and immunity monitored in order to compensate for viral evolution.
One thing about the anti-vaxxers I’ve interacted with - they absolutely do not believe the elites ever vaccinate themselves or their kids.
Unfortunately I can’t think of any way to prove it to anti-vaxxers short of them being in the room when Bill Gates gets the jab - and letting them choose a vial chosen out of a gigantic batch of vials. And even then it might sway only the people in the room.
Don’t forget “people are saying…”
I mostly agree but because I take care of moms I don’t want to take any chance of getting it and bringing it home, even if she is vaccinated. She has an extremely weak immune system so I have no idea how protected she will be.
I dunno I still feel gross about it and welcome any criticisms or people telling me I don’t need it and I’ll reconsider, but my NP nurse sister says I need it since I take care of mom.
2 Likes
It seems very clear that you ought to be getting the vaccine ASAP.
5 Likes
Some discussion in this thread too:
1 Like
Ok, I now remember this point. Good Luck in getting the vaccine. But, I would add no-one who’s had the vaccine has encountered a severe case of covid afterwards, so maybe she safe even if you were to bring it home.
On the other hand, seems like a free for all atm in the US so maybe ‘every man for himself’ mode ain’t too off the moral compass.
Ignore Churchill and listen to your sister. In fact, in some states you could probably be classified in a early group if you legitimately are caring for a disabled or severely ill person.
1 Like
I just found that the county website (Contra Costa) is taking requests for appointments for residents who meet certain criteria. You put in your info and they say that they will get back to you in a few days. So it seems like the wheels are in motion.
1 Like
IIRC not a whole lot of old sick people were in the test group.
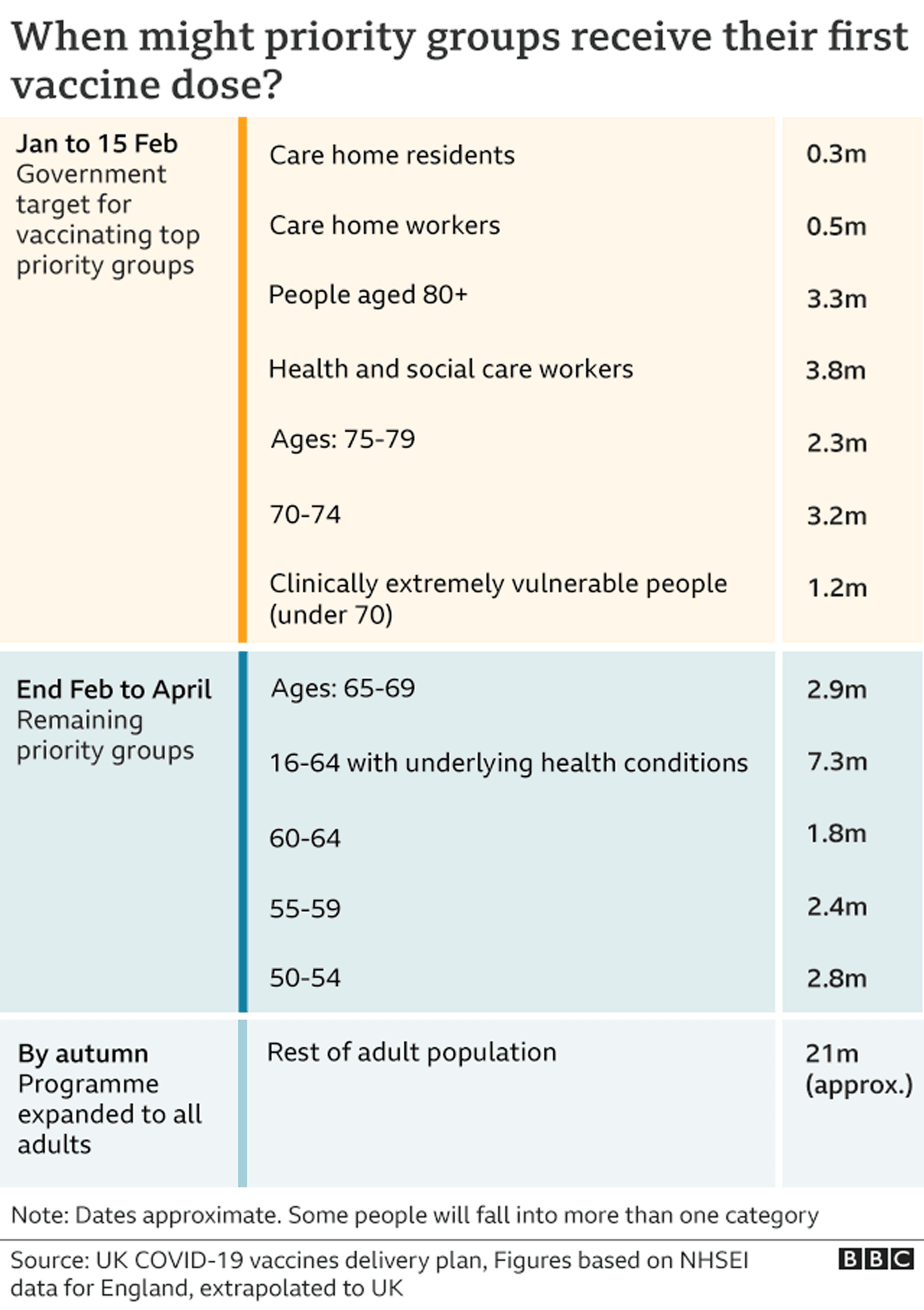
UK has been vaccinating mainly over 80yrs for the last 6 weeks - haven’t heard of any vaccinated cases dying yet - though I suppose it’s possible early after first dose.
I think if you don’t take it, another person not so close to a highly vunerable person might take it anyway, so, you know (I have COPD btw, probably not as severe as your Mom…yet)
Context: No one under 50yrs without a underlying condition vaccinated til May earliest in UK
People here may or may not remember my posting in the last year about learning via FB that one of my favorite high teachers is actually a POS deplorable.
In the last week, this 75 year old in CA with a Ph.D. wrote “I’m not getting the vaccine now if my wife can’t receive it as well.”
Potentially infecting the wife to own the libs!
1 Like
My tribal clinic went to phase 2 today. I’m scheduled for the Moderna jab Monday @2:30.
To recap, I, a unemployed 34 year old former smoker who is moderately overweight atm, am getting vaccinated before my 35 year old partner who works with COVID + bodies every day in a funeral home that is so overwhelmed they had to bring in a refrigerated trailer.
8 Likes
Freudian slip?
1 Like
I’m conflicted about stories like this:
Cliffs: Assuming it is reported accurately, this guy took a punctured vial at the end of the day (it will be unusable for the following day and all vaccine in it would be wasted) and vaccinated his friends and family with it (he alleges they are all people who would qualify under the rules anyway).
It’s not clear cut because they dispute what would have happened to the doses if he didn’t take the vial. I’ve looked at a few articles about this story. He claims they definitely would have been wasted. The health department says they have a protocol for what to do and they definitely would not have been wasted. I think the truth is that they would have likely but not definitely been wasted.
Assuming that the accused is correct in his assessment of what would have happened to the doses, I’m not sure what the right punishment is here. I feel like almost the whole range of possible responses could be justified.
lol people are still interacting with churchill
5 Likes
que?
Whoops. Didn’t mean to reply to you.
What Trolly said. You’re a frontline worker brother.
4 Likes