Okay, but you’re using IFR to estimate how many cases we had. You don’t want true IFR if everyone had it with perfect care provided in a situation with no stress on hospitals.
You want the IFR of cases in the US to date if you’re trying to estimate how many cases we’ve had in order to take a guess at how far we are along for herd immunity. That’s how this debate started, right?
Now if you’re just talking about the current IFR in ideal circumstances, that’s different.
All this IFR stuff is just as a sanity check for actual cases vs. confirmed cases. .3% could be accurate if at least nursing homes and some other high-risk people in ND are isolating well. Or maybe it’s still way too low. Who knows.
Is ND at least in the 25%+ ballpark of infected? Probably. Could it be as high as 50% infected? Maybe. Herd immunity with overshoot is maybe 80% infected? If this wave dies down then they have another smaller wave, the overshoot could be lower. Maybe 70% is herd immunity.
It’s a lot of maybes. But I feel confident ND is in the conversation for getting somewhere close to herd immunity by May - is my only point. Especially if you assume nursing homes will stay pretty safe/isolated until cases go to zero. Then throw some vaccine on that starting in late Dec. and cases could plummet pretty quickly. Or not.
IFR of the US is meaningless to me btw except as a ballpark on top of a ballpark. People’s health condition and average age vary so much from state to state. Looking at the data to the most granular level we have makes sense.
Even the IFR of LA county doesn’t make as much sense to me as breaking it down by region. Look at Manhattan vs. Queens and the Bronx.
The other factor though is whatever % of people tested positive with no symptoms may not have much immunity. And by a year+ maybe immunity starts to wear off in a big chunk of people. But ND didn’t have too many back last spring, so that’s good.
So many variables.
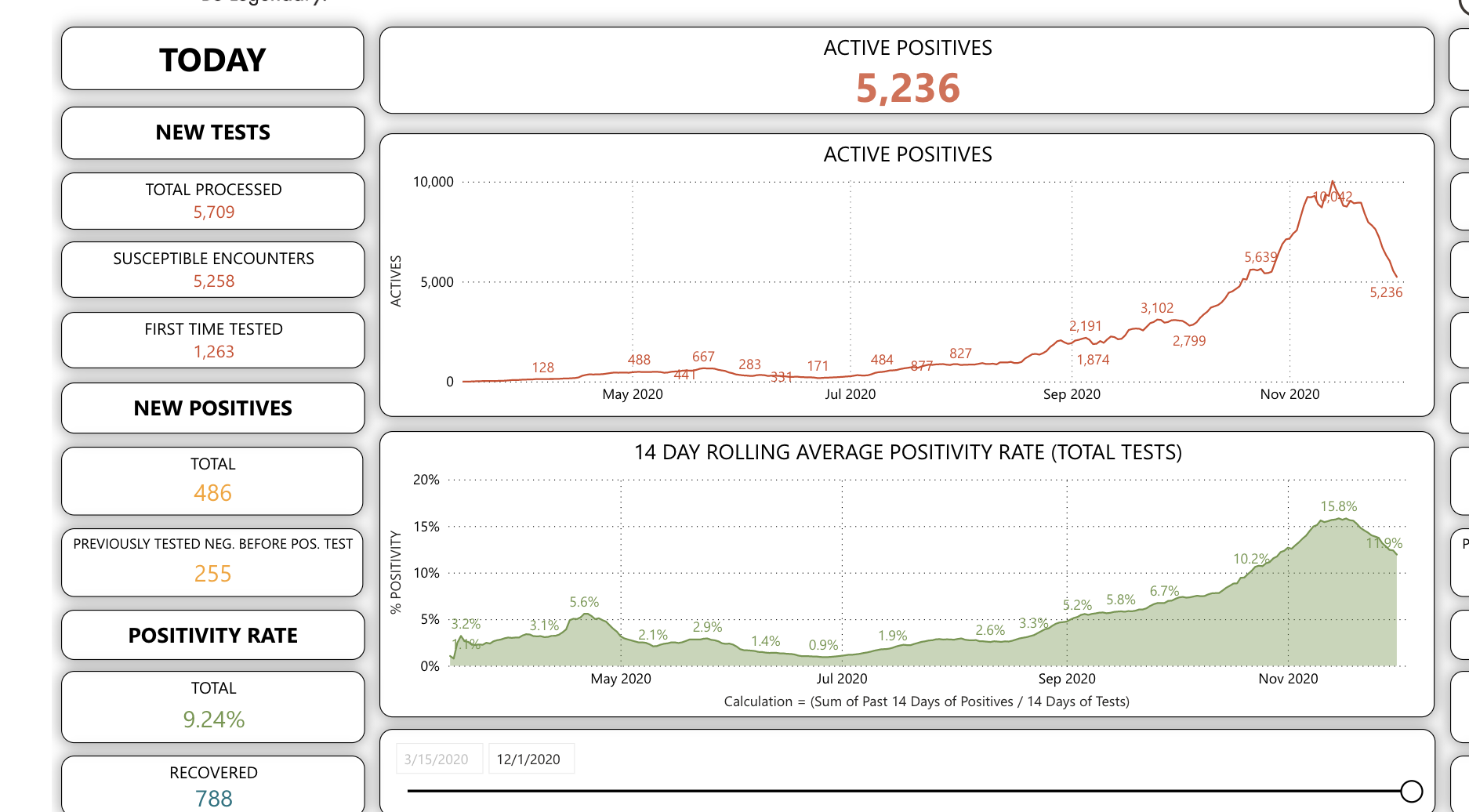
Currently sitting at 2nd highest case day and highest death day for Covid in the US and still a couple states to report. Seems not good.
North Dakota has 972 deaths and 762K people.
An IFR of 0.5% means 194K cases, or 25% of the population. At 50% you’re now going with 0.25% for the IFR.
I don’t know what to tell you man, I don’t think you’re being at all realistic with this stuff.
I’ve seen herd immunity estimates as high as 82%, and it’s likely to spread easier the next few months with everyone indoors.
I mean North Dakota is likely to get above 70% before a vaccine if not worse, but not because they’re currently close. Because they’re very… committed.
.25% IFR minus a 3-4 week lag. There are about 300 people in the hospital right now. In a month there may be 1100 deaths and 200 people in the hospital.
And again - if IFR doesn’t include nursing homes because they’re all locked down, and some other at-risk people, then it could be a lot lower than “true” IFR.
We are… We were going horizontal for a while, then we entered the corner, and we’re now rounding the corner and going vertical.
1 Like
Ok I’m really done with this thing I supposedly wasn’t going to get sucked into AGAIN.
There’s about 100 confounding variables here and a margin of error of like 100% either way. My bet is that ND will be in the conversation for something like herd immunity by May - and it won’t take much of a kick for vaccines to help that along. We’ll see what ND’s cases look like in Feb-April.
90M isn’t even halfway to herd immunity, unfortunately
Your estimates require orders of magnitude difference, which isn’t really possible.
Much like our discussion wrt to herd immunity, the issue here is that you don’t understand a term. You can’t adjust the IFR based on if nursing home isolates or not. That’s not an IFR anymore.
2 Likes
I’m saying they could get it sooner than that, but only because it’s going to keep doubling if they keep doing nothing.
Then give me a term for it? I’m not saying I’m talking about true IFR - which I thought I made super clear.
True IFR doesn’t even exist in practice since the first wave of Covid. Some people are always going to separate themselves from the pool. Same for herd immunity. And on top of that both are constantly changing as people’s behavior changes throughout the pandemic.
As has been discussed ad infinitum - there’s no such thing as true IFR or HI for human beings in late 2020 - except in theory. That should be a given in our discussions - no need to semantics me on IFR.
IFR wasn’t even part of my point. It was just a very rough sanity check to actual cases being 5x confirmed cases. Maybe it’s lower, which I totally allowed for.
I’m not saying anything less. But cases do seem to be dropping right now. They could be having a Manaus type behavior-modified (guessing, it’s still kind of a mystery but behavior is my best guess) dropoff, and a Manaus-type subsequent wave after they get complacent again wouldn’t surprise me.
Dropping or flattening? Could be testing capacity.
Never said it was. But it might be enough that vaccines put in more of a dent every month than say Taiwan or Vietnam - which are starting at effectively zero infected.
My point is our shittiness may mean we need less vaccine before we start to see a dropoff. Or maybe the already-infected effect won’t be that much at all. Just speculating on possible paths.
I did this to myself, again. I have no one to blame but myself, again. See you in a few days.
This isn’t correct either. The IFR is the risk of death if you plucked one random person from a given population and gave them covid. I don’t know what you mean by ‘true’ IFR. I think you mean fatalities over people infected. Again, that’s not correct.
It was higher than 1% in March/April if 0.2% are dead because 20% didn’t get it in NJ.
But that was early and an older population so expected to be higher than the blended average.