We travelled yesterday on lol American, and although things went mostly ok, we had multiple short delays related to short staffing at Reagan (DC). Things like nobody available to operate the jet bridge, nobody available to carry a bright stick and waive it around when the plane gets pushed back. Nobody available to bring the luggage over to the plane, etc. I figured since most of DC seems to be infected at the moment, it might have been related to that.
Thought it was odd that there was a line out the door for my gym at 8 AM this morning on Christmas Eve. Until I got closer and realized that it was the line from around the block for Covid testing. Absolutely insane that we still have to line up for hours two years into this thing.
1 Like
Well try to hang on until January sick folks.
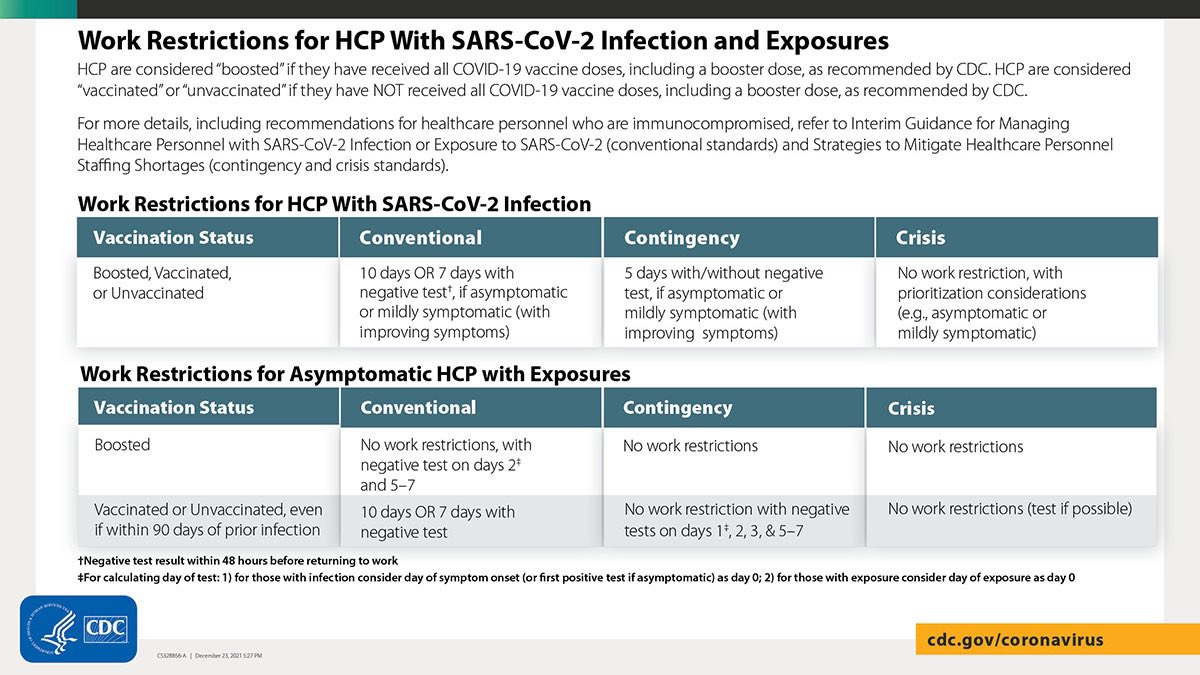
As expected, the plan for when the hospitals
fill is to put infected workers back into the rotation.
2 Likes
airlines have been trying to absolutely minimize this sort of ground staff for a while, even before covid, so these sorts of annoyance delays are pretty common.
for AA at DCA, that seems more likely to specifically be covid-staffing-related, though, since they have a pretty big operation there (not sure if it properly qualifies as a “hub” but it’s close) and the cuts are usually at outstations
Same problem happened with hydroxychloroquine and iver.mecti.n. Turns out that neither one worked that great (or maybe at all with the hydroxy). But we need an advocate for the drug, and the FDA obviously isn’t interested. There needs to be a mechanism for orphan drugs to get approved. Covid is a big enough deal that this will probably turn out to be OK, but there needs to be some sort of mechanism and funding for this sort of thing for non-covid diseases.
Man, even NYT is sweating your bets!
https://twitter.com/erictopol/status/1474387665847914500?s=21
2 Likes
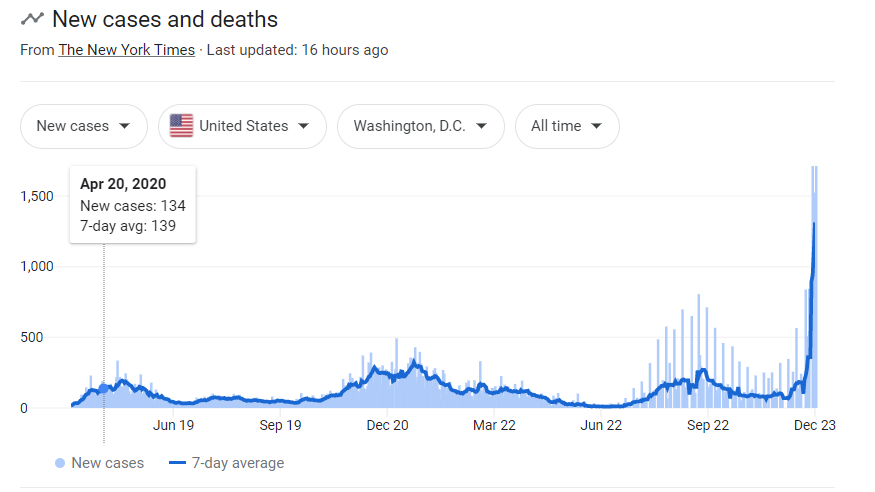
RSA’s 3-day trend has been downward, not sure if that’s due to testing errors or if this burns so fast that it’s running low on susceptible targets.
It’s going to be an interesting sweat from here. Basically can M-F next week, which should have huge numbers, outweigh the weekend/holiday. Yesterday “only” being in the 260s is good for me.
I don’t fly anywhere near as frequently as you, and have certainly experienced these kind of delays, but never all of them on the same trip. But DC is for sure having a normal one right now…
everyone has tested negative, including my sister’s 2nd test. So it seems most likely that her first test was a false positive? Seems incredibly unlikely that everyone else dodged it if she really is positive (I don’t think she really isolated from her husband/kids)
5 Likes
well, i tested negative since returning from my trip, but i still caught whatever flu/common cold was floating around, and it’s manageable but much worse than i remember seasonal plagues being. apparently my immune system isn’t primed after 2 years of self-isolation.
4 Likes
That’s certainly odd because we’d expect the at-home tests to miss toward false negatives, not false positives, and by a whole lot.
2 Likes
Quick google shows false negatives at ~15 per 100 and false positives at ~1 in 100, it’s not too crazy.
Despite this being considered a giant spike in America, there isn’t a single zip code in NYC with a 7 day case average per 100,000 higher than the Czech Republic’s total. Greenwhich Village is the highest at 349 while the Czech Republic as a whole is at 506.
And that’s down from a peak of over 1,300 a month ago. And I was teaching in that wave. Sure it sucks here but I’ve been through worse. Just doesn’t feel that way.
1 Like
Most of the ones I looked up actual data for were even lower false positive rate, but let’s assume 99% specificity which is still very good. What’s the sensitivity of RT-PCR?
I don’t know what testing capacity is like in the Czech Republic, but in NYC there have to be tons of people showing up to these lines and then going back home. I would guess positivity rate is a better comparison.
Here is what I am getting at: (1) Screen 1,000 pozzed and 1,000 unpozzed people with a lateral flow assay that has sensitivity 85% and specificity 99%. (2) Re-test the positives with PCR to confirm. I’ve set the PCR ROC to produce equal number of true and false negatives (sensitivity = 98.8%, specificity = 100%):
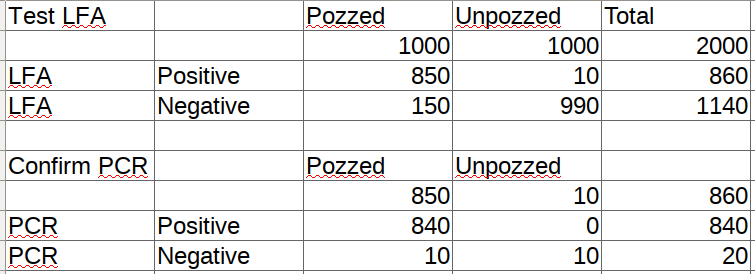
I dunno what the clinical performance of PCR is for covid detection but I assume it’s not quite that good in practice. The point is that, under these hypothetical starting assumptions, the answer to the question “What is the probability that a person who tests LFA positive and PCR negative actually has COVID?” is 0.5, and those individuals represent only 1% of the total starting population. However, the ratio of testing populations is unlikely to be 1:1 so can play around with that and the sens/spec to generate a range of plausible answers to that question.
Epi on twitter are emphasizing this too, for a green light you’d really need a PCR (good luck) with isolation post PCR then confirm with a rapid. So exposure plus a negative antigen test doesn’t make it safe to gather.
That said, US rules and recs are almost certainly about to head in a different direction I.e. 7 days iso and negative antigen gets you out given the IME forecast that like 40 percent of the population gets infected in the very short term.