By waiting a few months, they’ll gain an immense amount of data on exactly how harmful it is for a child to catch COVID, which will enable them to do a more informed risk analysis of the vaccines. Undertesting is a huge problem for understanding the severity numbers, but as the share of infected approaches unity, that problem goes away!
1 Like
are there any vaccines that have had “long term” negative effects, i.e. negative side effects that didn’t become apparent until years later? This is the most common objection I hear when people explain their hesitancy but every notable negative side effect I can think of with any vaccine ever is basically immediate.
3 Likes
One notable negative side effect of the vaccines I got as a kid is that now I’m alive to deal with stupid bullshit at work this week.
19 Likes
Nope. There have been vaccines where it has taken a bit for the realization that there are common short-term side effects. There was one of those discussed upthread. But a vaccine where you find out years later that lots of people who took it at getting super-cancer? Yeah, no, that’s not a thing.
1 Like
1 Like
I am kind of wondering whether the Czech Republic is at herd immunity levels. OWID says 48% of people are fully vaccinated, and 15.6% of people have had confirmed cases. If you assume testing is only catching a third of cases, that would give you 47% of the population infected. If catching COVID and getting vaccinated are independent, that means about 75% of the population has some form of immunity. That’s probably not quite herd immunity, but it could be enough immunity that mild restrictions are enough to keep a lid on Delta. I guess that’s a mildly optimistic take?
What is the latest on children vaccines? I have seen that they asked for more trials… they started trials in March… wtf is taking so long. Why are they asking for more trials 5 months later?
What is the basis of this number?
I mean it is possible. Late October - Early March 2021 we were basically getting torn apart by COVID. At least 0.1% of the population was getting covid per day at the peak of the wave. And on some of those days, over 40% of the PCR tests (including a couple over 50%) given were coming back positive which shows that our testing wasn’t adequate enough. So I’m sure there were cases missing.
Given how poorly we handled the virus, we’d be the prime example of what happens when a virus spreads almost unimpeded through a country. You get (formerly) the most deaths per capita and a ridiculous percentage of the population infected within some months before it dies out. At least that is until a new mutation gets around our current immunity.
It’s basically a guess. I had a hard time finding good seroprevalence studies. This paper estimates that the U.S. was detecting 23% of cases during our winter wave. So I basically just took that as 1 in 4 detected and cranked it up to 1 in 3.
It’s not going to be possible to come up with a useful estimate of that number though, so it probably makes more sense to look at it the other way around: what detection rate is compatible with the CR being at herd immunity, and is it plausible? The real evidence for possible herd immunity is that there’s no Delta wave.
Yes, this was a good article:
I feel like the CFR is still pretty constant, but what’s tricky is that when I look at that naive metric of deaths relative to lagged cases, I’m assuming a constant lag. But I think that’s probably not accurate - if Delta is more dangerous, I think it’s reasonable to expect that the lag might be shrinking. So this leads to a multiple hypothesis problem - I’m using the same metric to assess two different hypotheses, which is bad. [I could assume that the lag is constant and then test whether the CFR is changing. Or I could assume that the CFR is constant and test whether the lag is changing. But I have to make at least one assumption here. I’m choosing the first.]
There’s a way you could bake that shrinking lag into the estimated CFR if you thought you could measure it, but I haven’t tried to do that. So I’m in the camp of “I think the CFR has stayed fairly constant, maybe declined a little bit, based on my naive measure, but I’m happy to change my mind if I see more rigorous analysis.”
This seems very different from other countries. As Jordan put it:
I don’t think that chain is actually broken in the US. (I think it’s going to become pretty evident whether this is true in the next week or two, given that the most recent increase in cases really picked up in mid-July.) So how is it that CFR continues to be high if we have widespread vaccinations and the vaccines are very effective? I think where I’ve landed is:
- Primarily, vaccines are very effective in preventing cases, so the overwhelming majority of confirmed positive cases are among the unvaccinated. There’s no reason to think that unvaccinated individuals would have lower CFRs now than they did a year ago.
Then there are two offsetting effects:
- The age distribution of positive cases has shifted, so that a much larger percentage are among younger, lower-risk individuals than older, higher-risk individuals. Looking at aggregate CFRs (like I do), this will bias towards a lower CFR.
- The delta variant is more dangerous, so that on an age-adjusted basis you’re going to see higher death rates among the under 60 crowd in more recent months than you would earlier in 2021 or in 2020. That, all else equal, increases the CFR.
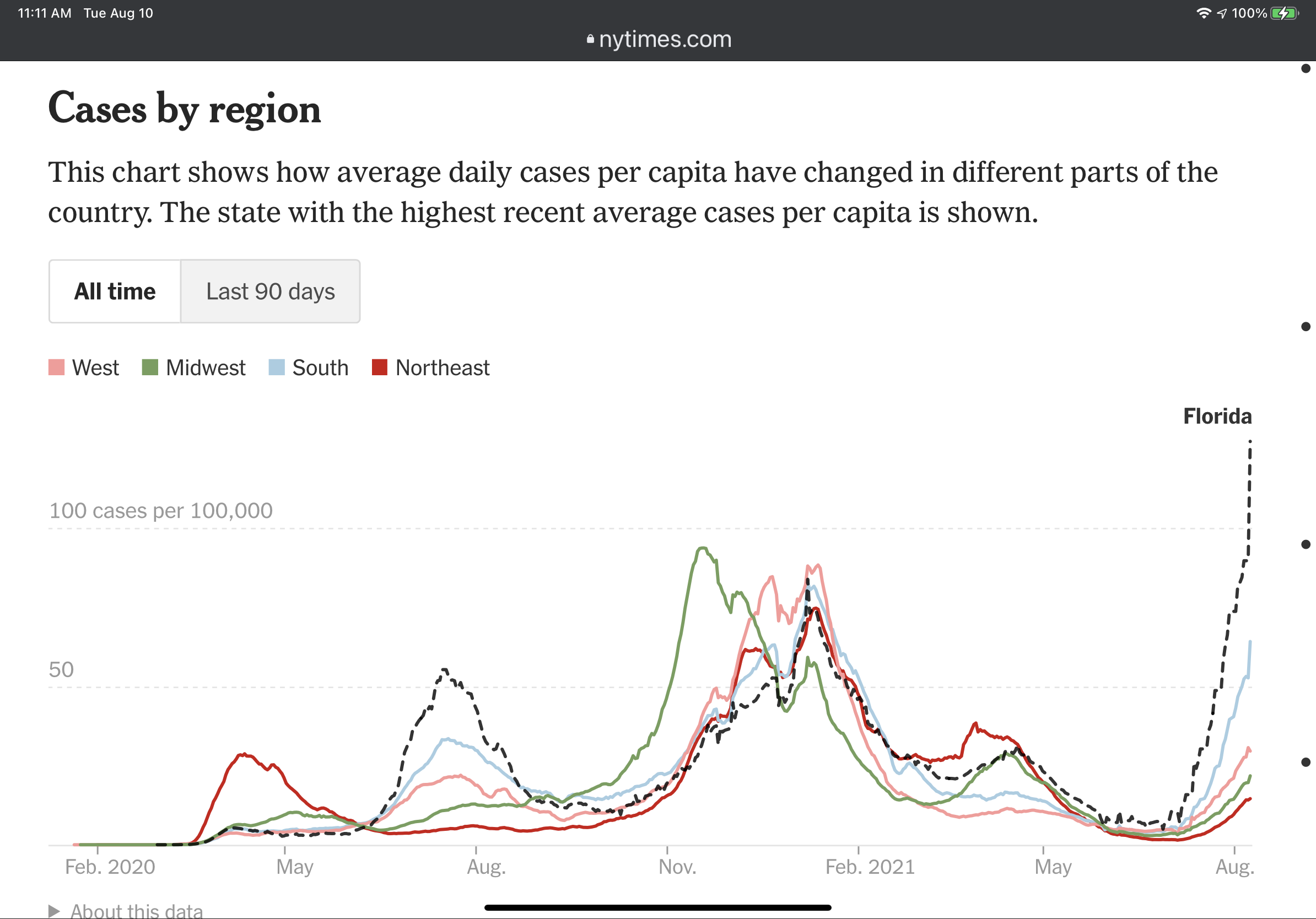
One of the things I’ve been wondering about, prompted by the obvious shitshow that is Florida, is the possible effect of localized vaccination rates. Say you took a large area and divided it into 50 sub-areas. In one experiment, you randomize vaccinations across the entire large area, so that every area experiences about the same rate of protection and presumed decline in spread. In another experiment, you intentionally vaccinate some sub-areas at a much higher rate, so that the community spread in those areas really declines, but the spread in the other areas is unaffected.
Do you end up with a different aggregate rate of cases under those two experiments?***
***This is so enormously stupid that I’m embarrassed to write it, but I think this question was prompted by baseball and the difference in expected runs between getting 4 total bases via a home run vs. 4 singles.
1 Like
How much of the death rate in America can be attributed to simply not having the resources necessary to treat everyone who needs lifesaving treatment?
One time a bad batch of 200000 Polio vaccines gave like 40000 people Polio. Not sure if those effects were immediately obvious.
low. only truly got close to being run over for about a week in nyc. Overused systems will still stress though and not be 100%

Cro Magnon Lady suspended one week
2 Likes
I hope he tears both ACLs on the same play
https://twitter.com/jamisonhensley/status/1424755160425897986?s=21
Wow. That’s great. Hope we hear more about this.
I tracked the offset by 7, 8, 9,… 28 days and used the point that was closest to where it more or less plateaud. Last year that was 21 days.
I have not tried with this year/delta. I’d have to build a whole new front end as the data is differently organized plus it’s so inconsistent across states currently.
If I had to pull an offset out of my hinie I’d say 14 days.
DeathSantis’s hitler youth are toddlers - he had them in a horrible tv ads building a wall with their legos - so i’m pretty sure that’s a trap.